
All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Skull base fracture
Medical expert of the article

Last reviewed: 12.07.2025
A basal skull fracture involves a fracture of the bones that form the basis of its outer surface (basis cranii externa), as well as the structures of the inner surface of the base of the skull (basis cranii interna). [ 1 ]
According to ICD-10, a fracture of the base of the skull has the code S02.1 and includes fractures of the temporal, sphenoid and occipital bones; cranial fossae formed by parts of various bones, the upper wall of the orbit (orbital plate of the frontal bone); sinuses of the ethmoid and frontal bones. [ 2 ]
Epidemiology
According to statistics, in cases of severe craniocerebral trauma, the frequency of basal skull fractures ranges from 3.5-24%, and they account for about 20% of skull bone fractures. 70% of fractures occur in the anterior cranial fossa and 20% in the middle.
The incidence of basal skull fractures in children after head injuries is, according to some data, 11%. [ 3 ]
In isolated injuries to the structures of the outer and/or inner surface of the base of the skull, the mortality rate reaches 29%; post-traumatic disability of varying degrees is observed in 55-60% of patients. Simultaneous fracture of the bones of the vault and base of the skull in almost 45% of cases leads to the death of the victims. [ 4 ]
Causes skull base fracture
The causes of basal skull fractures, as well as risk factors for damage to the integrity of the bone structures of its outer or inner surfaces, are significant craniocerebral injuries and head/neck injuries. They can be sustained by drivers, passengers and pedestrians in road accidents; in accidents at work and in many sports (primarily those associated with speed and extreme loads), as well as as a result of falls, severe bruises and direct blows to the head. [ 5 ]
A fracture of the base of the skull in infants is etiologically associated with head trauma from falls, and in newborns, such a fracture can be caused by trauma to the skull during childbirth (if the head is not brought out correctly).
As clinical experience shows, these fractures most often affect the petrous part (pyramid), crest and processes (styloid and mastoid) of the temporal bone; cranial fossae; areas of the sphenoid sinus, foramen magnum and occipital condyles. Such fractures can be isolated, but often with TBI the cranial vault is also affected, that is, a fracture of the bones of the vault and base of the skull is combined. See – Skull structure [ 6 ]
Almost 10% of basal skull fractures (particularly the occipital condyle) are associated with a fracture of the cervical spine (the upper two vertebrae of the craniovertebral zone).
A distinction is made between a closed fracture of the base of the skull in the case of a closed TBI, when the skin covering the fracture area is not damaged, and an open fracture of the base of the skull in the case of an open TBI with a rupture of the skin and exposure of the bone.
A fracture of the bones of the base of the skull may be comminuted - if the bone is crushed into separate fragments, and if the broken segments are displaced inward (towards the meninges and brain), the fracture is called depressed. A bone crack in which there is no displacement is defined as a linear fracture of the base of the skull.
A skull fracture with transition to the base is observed when the crack in the cranial vault continues onto the bones of its base.
A fracture of the base of the skull of the temporal bone often occurs, since its lower part is included in the base of the skull, the squamous part is the lateral wall of the cranial vault, and the anterior and posterior surfaces (together with parts of other bones) form the middle and posterior cranial fossae of the internal base of the skull. In addition, the temporal bone is an air-bearing bone, it is thinner than other bones of the skull (the frontal bone is 1.4 times thinner, and the occipital bone is 1.8 times thinner), has two processes (styloid and mammillary), and is also penetrated by several canals, canals, grooves and fissures. Read more - Fracture of the temporal bone [ 7 ]
Pathogenesis
As is known, the pathogenesis of any bone fractures is caused by significant mechanical (high-energy) impact, in which the bone is deformed and destroyed due to exceeding the limit of biomechanical properties of bone tissue (which has a layered-crystalline lamellar structure) - resistance to applied force (elasticity) and strength.
More information in the material - Structure and chemical composition of bones
Symptoms skull base fracture
The first signs of a basal skull fracture are determined by its location and the nature of the damage to the bone structures. But, in any case, the victim feels severe pain, dizziness and loses consciousness; vomiting may occur, and instability of blood pressure and heart rhythm (tachycardia or bradycardia) is noted.
If the fracture affects the petrous part (pars petrosa) of the temporal bone, blood accumulates in the tympanic cavity of the ears (hemotympanum) and bleeding from the external auditory canals is possible.
Rupture of part of the membrane of the brain during fractures of the base of the skull is associated with the leakage of cerebrospinal fluid from the nose or ears - liquorrhea, which in most cases is observed several hours after the injury. [ 8 ]
In addition, characteristic symptoms of such a fracture include retroauricular ecchymosis - intradermal hemorrhages behind the ears - in the area of the mastoid process of the temporal bone (Battle's symptom or sign), as well as around the eyes - periorbital ecchymosis (which is called "raccoon eye"). Ecchymosis in the retroauricular region and otoliquorrhea (cerebrospinal fluid leakage from the ears) are observed with a fracture of the middle cranial fossa (fossa cranii media), that is, the parts of the sphenoid and temporal bones that form it, and other manifestations of it are loss of sensitivity of the middle part of the face, impaired gag reflex, tinnitus and conductive deafness.
In patients with a fracture localized in the posterior cranial fossa (fossa cranii posterior) and the foramen occipitale magnum located in the occipital bone, vomiting, nasal cerebrospinal fluid leakage, and bleeding from the nose and ears, Battle's sign, and ecchymosis of the periorbital region are observed.
Hemorrhages in the eye area may indicate a fracture of the bones of the inner surface of the base of the skull, forming the anterior cranial fossa (fossa cranii anterior), which is also accompanied by anosmia (loss of smell), nosebleeds, hemorrhages under the conjunctiva and corneal edema, severe ophthalmoplegia (impaired eye movement) and drooping of the upper eyelid - ptosis. [ 9 ]
Complications and consequences
In case of fractures of the base of the skull (isolated or with a fracture of the bones of the vault), severe complications may arise and consequences may develop that may be irreversible.
Basal skull fractures can be complicated by meningitis due to the increased likelihood of bacteria entering from the paranasal sinuses, nasopharynx, and ear canal (since the fracture in many cases affects the pyramid of the temporal bone, the eardrum, and the ear canal).
Quite often, the integrity of the internal carotid artery is disrupted in the cavernous part of this vessel, resulting in the formation of an arteriovenous fistula – a direct carotid-cavernous anastomosis between the artery and the cavernous sinus of the dura mater.
The consequences include:
- pneumocephalus (intracranial air accumulation);
- cerebral edema with the development of intracranial hypertension;
- compression of the brain by bone fragments or subdural hematoma (formed as a result of subarachnoid bleeding);
- dissection, pseudoaneurysm or thrombosis of the carotid artery;
- damage to the cranial nerves (oculomotor, facial, vestibulocochlear), leading to neurological manifestations in the form of paresis and paralysis;
- cerebral coma.
Diagnostics skull base fracture
The diagnosis of a fracture of the bones of the base and vault of the skull is mainly clinical and is carried out according to the same algorithm as the diagnosis of traumatic brain injury, with a mandatory assessment of the severity of the injury.
Blood tests (general, electrolyte and oxygenation levels), as well as cerebrospinal fluid analysis and bacteriological culture are required to carry out antibacterial therapy.
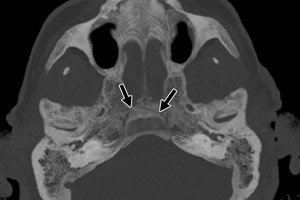
Instrumental diagnostics include X-rays of the skull and cervical spine, CT scans of the skull, magnetic resonance imaging (MRI) of the brain, and electroencephalography.
Differential diagnosis
In newborns, differential diagnosis includes congenital underdevelopment of the skull bones, intracranial hemorrhage (which may occur due to birth injuries), and encephalocele, which may be accompanied by cerebrospinal fluid leakage.
Who to contact?
Treatment skull base fracture
How first aid (pre-hospital) is provided at the site of the injury before the arrival of the medical team, and what needs to be done, is detailed in the publication - Help with traumatic brain injury [ 10 ]
After hospitalization of the victims, treatment is carried out in the intensive care unit and consists of anti-shock measures, stopping bleeding, supporting respiratory function, stabilizing blood pressure and heart rhythm (using appropriate medications). [ 11 ]
To relieve cerebral edema, dehydration is performed with diuretic injections. To prevent the development of meningitis when the infection enters the membranes of the brain, antibacterial drugs are used prophylactically (although the effectiveness of using antibiotics for prophylactic purposes has long been questioned). Read also - Treatment of traumatic brain injury
In cases of persistent cerebrospinal fluid leakage, as well as in cases complicated by vascular damage and intracranial bleeding, indentation of broken segments into the skull, compression of the brain, significant damage to the cranial nerves, surgical treatment is necessary – neurosurgical intervention with craniotomy. [ 12 ]
How long does it take for a basal skull fracture to heal? The healing process can take several months (a linear fracture heals much faster). At the same time, the rate of reparative regeneration, due to which bone fractures heal, may depend on the individual characteristics of patients and their growth. This refers to bone metabolism, the regenerative activity of osteoblasts of the cambial layer of the periosteum, as well as the intensity of bone tissue destruction by osteoclasts. [ 13 ]
Rehabilitation after a basal skull fracture, like rehabilitation after a traumatic brain injury, is carried out according to an individual plan - depending on the nature of the neurological, ophthalmological and other disorders that each patient has. Physiotherapy, exercise therapy, massage, speech therapy, etc. are used to restore lost functions and improve the condition. [ 14 ]
Prevention
Only prevention of traumatic brain injuries among all road users, during sports, in the industrial sector and at home can prevent a basal skull fracture.
Forecast
For patients with basal skull fractures, the prognosis depends on whether the fracture is displaced. Isolated, non-displaced fractures have a favorable outcome. However, in general, most patients with these fractures will have functional or neurological problems.
Most CSF leaks resolve spontaneously within 5 to 10 days, but some may persist for months. Meningitis may occur in less than 5% of patients, but the risk increases with the duration of the CSF leak. Conductive hearing loss usually resolves within 7 to 21 days.[ 15 ],[ 16 ]
After a fracture of the base of the skull (taking into account its severity), the survival rate is 48-71%, after a fracture of the bones of the vault and base of the skull - no more than 55%.