
All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
A heart study
Medical expert of the article

Last reviewed: 05.07.2025
Cardiovascular diseases are currently the most common. Their manifestations should be sought primarily during examination of the heart and blood vessels. However, a number of symptoms are found during a general systematic examination of the patient. Circulatory disorders caused by heart disease lead to the appearance of various symptoms, which can be associated with both ischemia and blood stagnation, as well as a systemic disease that has led to damage to the heart itself.
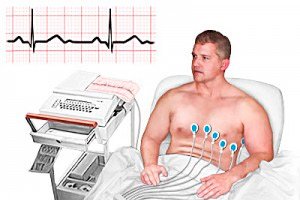
Advances in heart research have been achieved through the use of electrocardiography. The accuracy of heart disease diagnostics has increased with the use of X-ray contrast angiocardiography and invasive measurement of pressure in the heart cavities. Advances in non-invasive heart research are associated with the use of the ultrasound method - echocardiography.
However, despite the possibility of using highly informative instrumental methods, the decisive factors in the diagnosis of heart disease most often remain questioning and conventional physical examination methods, especially auscultation.
Questioning the patient is very important in recognizing heart disease. This primarily concerns complaints of pain in the heart or behind the breastbone, which, even in the absence of objective manifestations, often allows for the diagnosis of ischemic disease.
Medical history of heart disease
It is necessary to clarify with the patient the time of appearance of the main symptoms, their evolution under the influence of treatment, and the effectiveness of therapy.
It is important to establish how often and when periods of decreased working capacity occurred, whether disability was assigned and whether there were cases of hospitalization, especially in connection with hypertension and angina pectoris.
It is advisable to know the results of the clinical examination and the data of electrocardiography, echocardiography, as well as their assessment by the attending physicians. However, previously established diagnoses, such as a history of myocardial infarction, should be treated with caution. This also applies to the diagnosis of " heart defect " (this term is sometimes used by the patients themselves in the sense of the presence of heart damage).
It is important to clarify the reason for hospitalization and the patient's own assessment of the circumstances of hospitalization, since this largely determines the range of questions in differential diagnosis.
All questions related to the anamnesis (history) of life are clarified, including working and living conditions, lifestyle, bad habits, and in women - menstrual irregularities, use of contraceptives, past illnesses, and heredity.
As already mentioned, when conducting an examination and identifying certain symptoms, the doctor is especially forced to return to the anamnesis in connection with emerging questions and considerations. Thus, having identified angina pectoris and a history of heart attack, the doctor details the nature of the diet, focuses on the undesirability of excess nutrition and points out the need to replace animal fats with vegetable fats. If there is doubt about the presence of ischemic disease and to resolve prognosis issues, attention is paid to the so-called risk factors, which include the intensity of smoking and especially heredity (what parents and close relatives suffered from and at what age they died). It is very important, for example, to pay attention to the fact of the death of one of the parents from a heart attack at the age of up to 50 years or the development of heart pathology in a woman during menopause and at the beginning of menopause. Particular attention should be paid to the so-called alcohol anamnesis. At the same time, doubts may remain, especially regarding the durability of abstinence (refusal from alcohol) in the case of progression of heart failure in a patient with congestive cardiomyopathy.
For many patients, treatment details are important: dosage (for example, the diuretic furosemide), duration of drug intake, complications and symptoms of intolerance.
It is important to clarify the state of the nervous system not only from the point of view of the significance of the nervous factor in the development of the disease, but also its impact on the patient's quality of life. Treatment of arrhythmia, such as extrasystole, largely depends on how the patient tolerates it, i.e., including the sensitivity of his nervous system.
Questioning the patient is an extremely important element of his examination. It allows more often than using other physical methods to find key manifestations of the disease, which contribute to establishing a diagnosis and especially rational management (the nature of additional examination and treatment) of the patient.
 [ 1 ], [ 2 ], [ 3 ], [ 4 ], [ 5 ], [ 6 ]
[ 1 ], [ 2 ], [ 3 ], [ 4 ], [ 5 ], [ 6 ]
Complaints of heart disease
Pain in the heart area or behind the breastbone is a common complaint of patients. It is important to be able to distinguish between coronarogenic, or ischemic, pain caused by insufficiency of coronary circulation (angina, myocardial infarction) and cardialgia associated with damage to the heart muscle, pericardium and other causes.
The characteristics of pain in angina pectoris caused by acute myocardial ischemia are:
- localization behind the sternum;
- occurrence in the form of attacks during physical exertion, exposure to cold;
- compressive or oppressive character;
- rapid decrease and disappearance when taking nitroglycerin (under the tongue).
Peculiarities of questioning when identifying ischemic pain in the heart
- Do you experience any discomfort in your chest (behind the breastbone), arms, or neck?
- What is their nature (squeezing, pressing, stabbing, aching pain)?
- When did you first feel them?
- What do you do when you feel them?
- What causes them to appear (give examples)?
- How long do they last?
- What else is troubling you at the same time?
- Do they occur at rest: while sitting or during sleep?
- How often do they occur (several times a day, a week)?
- Has the pain become more frequent or severe in recent days?
- Do you take nitroglycerin for every attack, how quickly does it help?
- How many nitroglycerin tablets do you take per day (per week)?
Cardialgia (non-coronary pain) is usually localized in the area of the left nipple (or apex of the heart), has a stabbing, aching, cutting character, lasts from several seconds to many hours and even days, usually does not decrease with the use of nitroglycerin, and occurs in connection with various factors (rarely - with prolonged stress).
Both types of pain can radiate to the left shoulder, arm, shoulder blade. This is due to the spread of pain impulses along the nerve pathways and their projection in the brain.
It is important to highlight a group of diseases in which paroxysmal, intense, prolonged pain behind the breastbone or in the left half of the chest is accompanied by other serious symptoms, primarily a decrease in blood pressure. This applies to pain during myocardial infarction, thromboembolism of a large pulmonary artery, and dissecting aortic aneurysm.
However, there is most often no direct relationship between the intensity of pain and the severity and danger of the disease to life, i.e. severe (according to the patient) and prolonged pain can be experienced by a person without serious pathology, and vice versa, minor cardialgia can be a symptom of a dangerous disease.
Pain in the heart area (sometimes very intense) is often "caused by extracardiac causes. These include diseases of the lungs and pleura (pneumonia with secondary pleurisy, pneumothorax ), peripheral nervous system ( intercostal neuralgia ), digestive system ( reflux esophagitis ), inflammatory changes in the chondrosternal connections. Neurosis with signs of depression (in the absence of organic damage to the heart and other organs) is one of the common causes of cardialgia. Currently, there are dozens of diseases that cause pain in the heart.
Diseases accompanied by paroxysmal pain in the heart area
Cause |
Characteristics of pain |
Angina pectoris. |
A feeling of compression and pressure behind the breastbone for 2-3 minutes, associated with physical activity, food, eliminated at rest and after taking nitroglycerin. |
It intensifies with deep breathing, coughing, and is often combined with signs of pleurisy. |
|
Psychoneurosis. |
Associated with emotions, localized in the region of the apex of the heart, has a varied nature and duration (from 1-2 seconds to several hours). |
Disease of the esophagus. |
Burning behind the breastbone, more often at night in bed, is eliminated after eating, as well as nitroglycerin. |
It is provoked by movement and palpation of the vertebrae and persists for a long time after the end of the movements. |
|
Diseases of the chest (muscular, bone and joint). |
They are provoked by movement and palpation of the chest (especially the costal cartilages) and are of a long-term nature. |
Shortness of breath is a common manifestation of heart disease, associated with deterioration of its contractile function, i.e. heart failure. Shortness of breath in heart disease primarily occurs with physical exertion (walking, other muscle tension).
Dyspnea is a subjective sensation of shortness of breath or rapid breathing. The appearance of this sensation depends not only on changes in the function of the heart and lungs, but also on the sensitivity of the central nervous system, which perceives these changes through interoreceptors. The appearance of this sensation also depends on general fitness. In healthy, detrained individuals who are forced to maintain a sedentary lifestyle for a long time, dyspnea occurs with less exertion.
Attacks of sudden shortness of breath or suffocation may develop in patients with heart disease at rest, for example during a night's sleep or after intense exertion. These attacks are associated with acute left ventricular heart failure, with blood congestion in the lungs. In this case, the patient takes a sitting position.
Cough and hemoptysis may be associated with heart disease as well as a result of blood stagnation in the lungs against the background of left ventricular failure. Cough, usually dry, may precede the appearance of dyspnea. It may occur with an aortic aneurysm, leading to compression of the trachea or bronchi.
Palpitations and irregularheartbeats occur due to an increase in the number of heartbeats or their irregularity, i.e. arrhythmia. The sensation of palpitations, like other complaints, is subjective and can occur with a very slight increase in rhythm due to increased heart contractions.
Syncope, or fainting (attacks with impaired consciousness or dizziness) may be associated with a disorder of cerebral circulation as a result of a disturbance in the heart rhythm (its significant slowing down) or an episodic decrease in cardiac output into the aorta against the background of an existing narrowing of its orifice.
Rapid fatigue is a characteristic symptom of serious heart diseases, usually occurring against the background of heart failure. But it can also be a consequence of general intoxication during the inflammatory process.
Pain and heaviness in the right hypochondrium may be combined with swelling of the shins and are a consequence of heart failure and blood stagnation in the systemic circulation. Nausea and vomiting may be added to these manifestations, especially with rapid development of failure. These symptoms are possible due to an overdose of a number of cardiovascular drugs, in particular cardiac glycosides (digoxin, etc.). In general, most complaints are associated with cardiac dysfunction, such as heart failure and arrhythmia. A special place among the complaints is occupied by periodically recurring pain, the coronary nature of which is clarified by detailed questioning.
Who to contact?