
All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Contracture of the masseter muscles
Medical expert of the article

Last reviewed: 04.07.2025
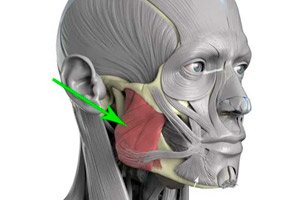
Long-term tension and contraction of the muscles that ensure movement of the lower jaw during chewing (musculi masticatorii) is diagnosed as contracture of the masticatory muscles.
Epidemiology
Clinical statistics on cases of contracture of the masticatory muscles are not available, but it is known that, for example, temporomandibular joint syndrome (TMJ) is detected in approximately 10-15% of adults who seek medical attention for craniofacial pain.
Causes contractures of the masseter muscles
The movements of the lower jaw during chewing of solid food involve the superficial and deep masticatory muscles (musculus masseter), which connect to the lower jaw bone and zygomatic arch; the temporal muscles (musculus temporalis) - anterior, middle and posterior; the medial and lower lateral pterygoid muscles (musculus ptrerygoideus). All these muscles are bilateral and are innervated by the mandibular nerve, which is a branch of the trigeminal nerve. [ 1 ]
The following main causes are noted that lead to contracture of the musculi masticatorii:
- fracture, dislocation and subluxation of the lower jaw (including habitual);
- problems with the dental system - violation of occlusion (closure) of the teeth, that is, malocclusion (maxillary or mandibular prognathism);
- temporomandibular joint disorders – temporomandibular joint syndrome (TMJ), the movement of which is provided by the masticatory muscles;
- myositis – inflammation of muscle tissue;
- tendinitis of the temporal muscle - inflammation of its tendons, which may be associated with hyperactivity of this muscle;
- defects of the mandible, such as hyperplasia of the coronoid process and angle of the mandible;
- facial hyperkinesis, in particular, abnormal movements of the lower jaw (oral hyperkinesis) - bruxism, "lower" Bruegel syndrome, tardive orofacial dyskinesia, oral masticatory syndrome (hemimasticatory spasm) in the elderly;
- spastic paralysis of the facial muscles (facial hemispasm);
- soft palate paralysis;
- Damage to the mandibular nerve.
Types of contracture of the masticatory muscles
There are different types or kinds of contracture [ 2 ]:
- post-traumatic contracture of the masticatory muscles,
- inflammatory contracture of the masticatory muscles (with fever, diffuse facial edema and craniofacial pain);
- post-paralytic contracture of the masticatory (and facial) muscles in cases of cerebrovascular accidents as a result of stroke - with damage to the upper motor neurons and the development of spastic muscle hypertonicity and facial hemispasm;
- neurogenic contracture of the masticatory muscles, for example, in patients with epilepsy or pseudobulbar palsy, which is the result of damage to the central motor neurons and corticonuclear tracts of the brain.
Risk factors
When determining the risk factors for the development of contracture of the masticatory muscles, specialists primarily emphasize the role of maxillofacial injuries, dental/orthodontic manipulations and local infectious processes (periostitis, pericoronitis, infection at the site of eruption of the third molar, other inflammatory foci in the oral cavity and nasopharynx), which can lead to inflammation of the masticatory muscles, as well as muscular dystrophy/dystonia and autoimmune muscle tissue diseases (polymyositis).
The risk of contracture of the musculi masticatorii with dysfunction of the masticatory system is increased in epilepsy, pseudobulbar paralysis and chronic stress. Thus, stress-induced tension in many people is accompanied by involuntary motor activity of the jaw muscles with clenching or grinding of the teeth - bruxism (from the Greek brykein - to bite or grind the teeth). [ 3 ]
But it should be borne in mind that long-term use of antipsychotic drugs can lead to a side effect in the form of neuroleptic syndrome, which is characterized by a tonic spasm of the masticatory muscles - trismus (from the Greek trismos - creaking). [ 4 ]
By the way, it is trismus that can cause shortening of the immobile muscle fibers of the pterygoid, temporal and masseter muscles and chronic limitation of their mobility.
Pathogenesis
In case of fractures of the lower jaw or facial bones to which the masticatory muscles are fixed, in cases of dislocations of the neck of the condyle of the lower jaw, the pathogenesis of contracture can be caused by the formation of a hematoma, focal rupture of muscle fibers, persistent muscle spasm (trismus), as well as structural changes in muscle tissue - with the formation of adhesions and scars, that is, fibrosis (fibrodysplasia), and even ossifying traumatic myositis.
Thus, contracture develops when normally elastic tissues are replaced by inelastic fibrous tissue, which tightens the muscle.
Studies have shown that structural changes in muscle tissue consist of greater rigidity – due to increased passive mechanical tension. In this case, the tension of muscle fibers is accompanied by stretching of sarcomeres (functional muscle units consisting of contractile proteins myosin and actin, combined into myofilaments), which leads to their functional inferiority, and the generation of active tension in the muscles decreases, causing rigidity (stiffness of movement).
Symptoms contractures of the masseter muscles
In case of contracture of the masticatory muscle, the first signs are limited ability to open the mouth. Acute pain in the masticatory muscle and tilt of the jaw towards the affected side (asymmetry of the lower part of the face) occur.
At a later stage, pain (dull or aching) may also be present at rest, radiating to the ear and temple area.
Symptoms also include a constant feeling of tightness and stiffness of muscles (due to their hypertonicity); difficulty eating (impossible to bite off and chew); problems with brushing teeth, yawning, articulation; clicking in the temporomandibular joint, muscle fasciculations are possible.
Complications and consequences
Complications and consequences of masticatory muscle contracture include painful muscle spasm and limitation of temporomandibular joint function and mandibular mobility, which may be referred to as facial myofascial pain syndrome, masticatory myofascial syndrome, Costen's syndrome, or facial pain dysfunction syndrome.
Diagnostics contractures of the masseter muscles
The diagnosis of contracture begins with examination of the patient and collection of anamnesis.
Laboratory tests may be needed - blood tests for lactate, lactate dehydrogenase and creatine phosphokinase levels.
Instrumental diagnostics include panoramic radiography of the lower jaw, CT of the maxillofacial region and temporomandibular joints, ultrasound of the muscles, and electroneuromyography. [ 5 ]
Differential diagnosis
Differential diagnostics are carried out with arthrogenic contracture of the lower jaw, arthrosis, neoplasms localized in the jaw area, trigeminal neuralgia, Bell's palsy (neuritis of the facial nerve), etc.
Who to contact?
Treatment contractures of the masseter muscles
Treatment should be aimed at eliminating the underlying causes. A partially impacted tooth may require extraction; orthodontic treatment is performed in case of malocclusion; antibacterial therapy is prescribed in case of infection; surgical treatment (by an oral surgeon or maxillofacial surgeon) is required in case of injuries and some anatomical defects of the lower jaw.
To relieve inflammation and pain, NSAIDs are recommended – non-steroidal anti-inflammatory drugs, for example, Ibuprofen (0.2-0.4 g three times a day), or other tablets for muscle pain.
To reduce muscle tone, drugs from the muscle relaxant group are used in small doses, for example, Tizanidine (Sirdalud). Side effects of the drug can manifest themselves in the form of increased fatigue and drowsiness, dizziness and arterial hypotension, dry mouth, nausea.
Physiotherapeutic treatment is carried out using the method of medicinal phonophoresis (with NSAIDs). At home, you can make wet hot compresses (several times a day for 15-20 minutes). Heat helps reduce pain and stiffness by relaxing muscles and increasing blood circulation in them.
Medical rehabilitation for contracture of the masticatory muscles after the inflammation has been relieved is aimed at restoring their normal function and includes – in addition to physiotherapy – therapeutic exercises and massage of the masticatory muscles.
Prevention
Preventive measures include timely treatment of inflammatory diseases of the oral cavity and nasopharynx, as well as prevention of occlusion disorders in children and, if possible, correction of malocclusion.
Forecast
In case of contracture of the masticatory muscles, the prognosis depends entirely on the cause of its occurrence. When shortening of muscle fibers is caused by excessive use, overload or physical impact and is within physiological limits, it is reversible. Contractions due to severe injuries, in which a significant part of the tissue of the muscle-tendon structures is destroyed, can be irreversible.