
All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Ultrasound signs of muscle tissue pathology
Medical expert of the article

Last reviewed: 04.07.2025
Muscle tissue pathology.
Muscle injury due to compression, impact (contusion). As a result of external compression of muscle tissue against bone, muscle contusion occurs. During longitudinal scanning, the damaged area looks like a cavity with uneven contours and echogenic contents. Healing occurs slowly, with the formation of coarse scar tissue and significant loss of muscle function later. Ossifying myositis occurs in approximately 20% of patients with this type of injury.
Strain. The first stage of muscle injury is overstretching. Typically, less than 5% of all the fibers in the muscle cross-section are damaged during a stretch. Clinically, the patient cannot pinpoint the pain point, complaining of muscle pain during contraction. Cross-sectional sonograms show micro-tears that look like multiple cystic areas.
On longitudinal scanning, micro tears have an elongated shape. On MRI on T2-weighted images, this is manifested by thickening of the muscle and an increase in signal intensity due to perifascial edema. Treatment consists of limiting movement and pain relief.
Partial tear. A partial tear is also caused by overstretching. In this case, more than 5% of the muscle tissue is damaged, but not throughout its entire length.
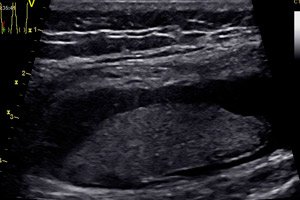
The muscle function is completely absent at the time of injury and partially returns after some time. Unlike a sprain, the patient clearly indicates the painful point, where, as a rule, there is swelling. Ultrasound examination clearly reveals a violation of the integrity of muscle fibers at the site of greatest pain. The damaged area of muscle tissue is replaced by a hypoechoic hematoma. The typical fibrous pattern disappears at the site of rupture. When pressing with a sensor, it is possible to visualize floating torn ends of muscle fibers. Muscle contraction allows differentiating the damaged muscle from an echogenic hematoma (at a late stage). During a dynamic examination, hyperechoic granulation tissue and regenerating muscle fibers appear at the site of rupture. On T2-weighted images, this is manifested by muscle thickening and an increase in signal intensity due to edema, hemorrhage, perifascial edema, or hemorrhage. Sometimes a muscle tissue defect is visible as a hyperintense band. In case of significant tears, surgical restoration of the integrity of muscle fibers may be required.
Complete rupture. Complete muscle ruptures are less common than partial ruptures. Muscle ruptures occur at the junction of the muscle and tendon. Clinically, complete ruptures are similar to partial ruptures. There is a complete loss of muscle function. The torn proximal end of the muscle contracts and can be palpated. With a complete rupture, there is a complete absence of muscle fibers, especially noticeable when compared with the contralateral side.
The muscle contracts and a hematoma forms in its place. In transverse scanning, the contracted echogenic muscle is surrounded by a hypoechoic rim. In frontal sections, when constructing a three-dimensional reconstruction of the pathological zone, the rupture can be visualized along its entire length. Treatment consists of surgical restoration of the integrity of the muscle.
Healing of muscle tears. Healing of muscle tears can take from 3 to 16 months, proportional to the extent of the tear. Muscles have a good ability to regenerate. Large muscle tears are accompanied by both regeneration and scar tissue formation. The goal of therapy is to support the regeneration process and suppress scar formation, which reduces regeneration. The role of ultrasound is to measure the tear and divergence of muscle fibers, as well as to determine the stage of the tear.
Initial changes include increased echogenicity of muscle tissue in the area of torn ends, as well as an increase in the size of this zone, which can be easily traced sonographically. Later, the feathery muscle structure becomes increasingly visible with a reduction in the size of the hematoma. Ultrasound monitoring of muscle structure recovery is very important. It can be used to control the timing of the start of physical activity. Early restoration of physical activity leads to repeated injuries. Longer limitation of mobility leads to excessive scarring. Ultrasound examination also includes the assessment of scar tissue at the site of rupture. In muscle injuries resulting from contusion, the scar has a stellate or irregular shape, while in ruptures resulting from overstretching, it is linear. The risk of repeated injuries increases with significant sizes of fibrous tissue, which sonographically appears as a local zone of increased echogenicity in the structure of muscle tissue. Muscle strength decreases in proportion to the size of the scar tissue. One of the complications after muscle rupture is the formation of muscle cysts. Treatment consists of excision of the cysts.
Hematoma. In the acute stage, the echogenicity of the hematoma is comparable to the echogenicity of the muscle. After 3 days, the echogenicity of the hematoma decreases. Due to lysis, late hematomas look almost anechoic with the presence of fibrin threads.
Sometimes, with an unfavorable course, an abscess may develop, which is characterized by the presence of a hypoechoic area with hyperechoic inclusions and pronounced perifocal blood flow.
On MRI scans, the signal intensity from a hematoma depends on its age. The signal intensity of a hematoma changes: from hyperintense on the first day to hypointense on the second; it returns to hyperintense by the end of the first week and lasts for up to three weeks; then it becomes hypointense again after a month. Such changes occur due to the conversion of hemoglobin into oxyhemoglobin, then into deoxyhemoglobin, methemoglobin, and hemosiderin with ferritin. An acute hematoma (1-4 days) has a medium and low-intensity signal on T1 and T2-weighted images. Subacute hematomas (4-7 days) are hyperintense on T1-weighted images, just like fat. Therefore, using fat-suppressed scanning programs, fat can be easily differentiated from blood.
It should be remembered that due to the bleeding of the hematoma, heterogeneity of signal intensity may be observed. On T2-weighted images, subacute hematomas are hypointense. In old hematomas (14-21 days), due to the conversion of iron from methemoglobin to hemosiderin and ferritin, the walls have low intensity on T1 and T2-weighted images and appear on MR tomograms as a hypointense "halo" around the hematoma.
Myositis. This is an inflammation of muscle tissue that can occur as a result of trauma, infection, or systemic disease. In viral infections, myositis manifests itself as myalgia. The inflamed muscle is sharply painful, enlarged, and dense to the touch. Muscle fibers become hyperechoic in comparison with the contralateral side. Fibrous layers stretched by inflammatory exudate become hypoechoic. Ultrasound angiography shows increased vascularization of the inflamed muscle. Perifocally, lymphadenopathy may be observed. An abscess may subsequently form - then the process is called pyogenic myositis. Typical picture: a cavity in the center of muscle tissue with heterogeneous contents. Clinical signs: pain, fever, leukocytosis, increased ESR.
Muscle atrophy. Muscle atrophy occurs due to many reasons. Chronic dysfunction of the joint, denervation, myopathy are the most common reasons leading to atrophy. It is manifested in a decrease in the volume of muscle tissue, when compared with the contralateral side. In ultrasound, an increase in echogenicity occurs due to fatty infiltration. On MRI, fatty infiltration of muscle tissue is also clearly visible on T1-weighted images.
Muscle fascia ruptures. Muscle fascia ruptures occur when overstretched. This type of damage is very specific for some muscle groups. For example, muscular-aponeurotic damage between the gastrocnemius and soleus muscles, soleus and the long flexor muscle of the big toe. The rupture zone is filled with a linear hematoma along the aponeurosis. A characteristic ultrasound sign is a violation of the orientation of the fibrous-fatty layers during longitudinal scanning. This type of rupture is very often accompanied by venous thrombosis.
Muscle hernias. Fascial defects appear as local protrusions of muscle tissue. Chronic muscle infringement most often leads to the formation of hernias, less common are post-traumatic and postoperative hernias. An ultrasound examination can reveal a fascial defect and hernial protrusion of the muscle. Often such hernias are detected at the site of perforation of the muscle by the vascular-nerve bundle. For example, along the outer surface of the lower part of the knee joint at the exit of the superficial peroneal nerve.
Hernias of the white line of the abdomen, inguinal, femoral can be detected. The pressure of the sensor on the skin during the examination of hernias should be minimal.
Thickening of the muscle fascia. Thickening of the muscle fascia can also affect muscle function. Shin splints are a condition in which pain occurs in the muscles of the front of the shin after excessive physical activity.
"Runner's knee". Friction syndrome arising in the iliotibial tract is another pathology of the fascial sheaths, the so-called "runner's knee". Clinically accompanied by pain in the lateral part of the knee joint at the site of the passage of the iliotibial tract fibers through the lateral femoral condyle. Running with obstacles or over rough terrain leads to the development of this syndrome. It manifests itself in thickening of the iliotibial tract fascia fibers, a decrease in their echogenicity immediately after running. In a calm state, these manifestations may subside.
Plantar fascia tears. Long-distance runners, marathon runners often suffer from foot pain. Heel pain occurs with fasciitis, which often causes heel spurs. The fascia thickens where it attaches to the calcaneal tuberosity.
This process is usually bilateral, so comparison with the contralateral side does not yield results. Ruptures appear in the middle part of the fascia and appear as a hypoechoic defect. It is necessary to differentiate ruptures from plantar fibromatosis.
The latter appears as a spindle-shaped thickening of the fascia with preservation of the fibrous structure. Plantar fibromatosis can occur in patients with Dupuytren's contracture, Peyronie's disease, superficial fibromatosis.
Useful links
Muscles https://ru.wikipedia.org/wiki/%D0%9C%D1%8B%D1%88%D1%86%D1%8B