
All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Thyroid adenoma
Medical expert of the article

Last reviewed: 05.07.2025
A benign neoplasm that forms in the tissue structures of the thyroid gland is a thyroid adenoma.
This disease occurs against the background of increased production of thyroid hormones, resulting in hyperthyroidism, and inhibition of the synthesis of pituitary hormones responsible for thyroid function.
The pathology most often develops in females, especially at the age of 45-55 years, and ecology plays a decisive role in the development of this neoplasm.
Such a tumor rarely becomes malignant, but this does not mean that it does not need to be treated. Adenoma causes a lot of trouble and discomfort, affects the overall hormonal background, and in some cases it still becomes malignant, so treatment should be prescribed as soon as possible.
Causes of thyroid adenoma
Regarding the causes of thyroid adenoma, the following can be said: unfortunately, they have not yet been thoroughly substantiated. There are only assumptions that the tumor appears as a result of increased secretion of a hormone produced in the anterior lobe of the pituitary gland, or during a period of vegetative disorders (when there is an incorrect flow of regional sympathetic innervation).
It should be noted that when there is a failure in the system of interaction between the pituitary system and the thyroid gland, a large tumor rarely forms: with an excessive increase in the amount of thyroid hormones, the secretory activity of the pituitary gland decreases, and the neoplasm gradually decreases in size.
In addition, specialists have identified possible factors that can cause the formation of adenoma in thyroid tissue. Here are some of them:
- hereditary factor (the possibility of a predisposition to the disease being inherited cannot be ruled out);
- unfavorable environmental conditions (excessive radiation levels, lack of iodine compounds in drinking water, air pollution from industrial waste and exhaust gases);
- constant and long-term intoxication of the body (harmful production, etc.);
- hormonal imbalance due to stress, illness, etc.
Symptoms of thyroid adenoma
Most adenomas have a latent, asymptomatic course. However, sometimes you can pay attention to the following symptoms:
- spontaneous weight loss not associated with diets or increased physical activity;
- unmotivated irritability;
- the appearance of intolerance to hot climates, which was not previously observed;
- increased heart rate, regardless of the presence of stress (the heart “beats” even during sleep);
- constant fatigue, even in the absence of physical work.
As the disease progresses, problems with the digestive system arise, blood pressure may increase, and sometimes (not always) the temperature rises.
Often, with a relatively latent course of the disease, the only signs may be drowsiness and increased heart rate at rest. However, over time, the symptoms will expand, and the cardiovascular system disorders will worsen: heart rhythm disturbances and dystrophic changes in the heart muscle appear. The result of such changes may be heart failure.
Adenoma of the right lobe of the thyroid gland
Normally, the thyroid gland consists of the right and left lobes and the isthmus. The lobes are adjacent to the trachea on both sides, and the isthmus is closer to the anterior surface of the trachea.
In a normal state, the right lobe may be slightly larger than the left, but this does not affect the development of the neoplasm in the right lobe.
According to statistics, one of the two lobes of the thyroid gland is most often affected, less often – the entire gland. Moreover, the right side is affected more often than the left. Meanwhile, the greatest danger is posed by a tumor of the isthmus, which has a much higher percentage of transition to a malignant state.
An adenoma of the right lobe of the thyroid gland, if it is large, can cause an aesthetic defect in the neck area, below and to the right of the Adam's apple. This symptom can initially be noticed only when swallowing. In this case, damage to the left lobe of the thyroid gland produces the same symptom on the left side.
 [ 3 ]
[ 3 ]
Adenoma of the left lobe of the thyroid gland
The left lobe of the thyroid gland is usually somewhat smaller in size than the right lobe. The tumor may appear on either side of the gland, but according to statistics, tumors of the left lobe may be somewhat smaller in size than nodes on the right side. However, an adenoma of the left lobe of the thyroid gland can be determined by palpation, a slight deformation is observed in the neck area, and a feeling of discomfort often occurs in the throat. If the tumor reaches large sizes, then shortness of breath, dilation of the veins of the neck, and difficulty swallowing are added to the listed symptoms.
Treatment and diagnostic procedures are prescribed regardless of which part of the thyroid gland is affected.
[ 4 ]
Where does it hurt?
Types of thyroid adenoma
Toxic thyroid adenoma (Plummer syndrome) is the formation of one or more nodular formations that excessively produce thyroid hormones. Such a neoplasm has a round or oval shape, has a small volume, but is determined by palpation. Cell growth can accelerate with an increase in the level of iodine in the bloodstream: simultaneously with growth, the amount of pituitary hormones also increases. After the tumor is detected, further tactics largely depend on its size: a neoplasm up to 20 mm can be treated conservatively, and neoplasms with larger sizes are preferably surgical. If there are many nodular formations and they are distributed over the entire surface of the thyroid gland, then a complete resection of the gland is performed. Thyrotoxic thyroid adenoma can occur in an existing non-toxic node.
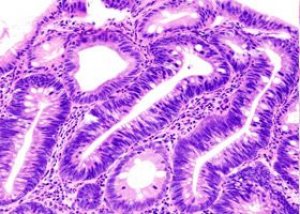
Follicular adenoma of the thyroid gland is often detected at a young age. Such a neoplasm originates in follicular cells, hence the name. The follicular form, in turn, is subdivided into trabecular, fetal, simple and colloid (depending on what other cells are present in the tumor). The follicular tumor has a spherical shape in the form of a capsule with a smooth surface and a dense structure. The capsule is subject to free displacement during laryngeal movements. Basically, follicular cells are benign, but in 10% of such pathologies, malignant adenocarcinoma is subsequently diagnosed. The difficulty is that at the initial stage, the tumor is difficult to detect: the follicular type does not produce hormones, and for this reason it develops unnoticed. Few patients consult an endocrinologist, feeling increased sweating, a constant desire to sleep and weight loss. Most often, people turn to doctors when the tumor begins to press on the esophagus and respiratory tract.
Papillary adenoma of the thyroid gland is a cyst-like formation containing dark liquid contents and papillary growths on the inner walls.
Oncocytic adenoma of the thyroid gland (second name: Hürthle cell adenoma) - occurs more often in women aged 20-30 years suffering from autoimmune thyroiditis. The pathology mainly has a latent course, only the clinical picture of thyroiditis - decreased thyroid function - can be observed. The neoplasm itself looks like a yellowish-brown tumor, often with small hemorrhages, consisting of several cell types. This disease is often mistaken for a cancerous tumor.
Atypical thyroid adenoma - a characteristic feature of the atypical form is the presence of various follicular and proliferating cellular structures with a round, oval, oblong and spindle-shaped form. Cell nuclei are hyperchromatic, while the size of the cytoplasm is often smaller than the size of the nuclei. This type of neoplasm can become malignant: in such cases, malignant cells can be observed under a microscope.
Oxyphilic adenoma of the thyroid gland is the most aggressive thyroid tumor, in which the risk of malignant transformation is extremely high.
Most nodular formations in the thyroid gland are benign. They can have a dense consistency or resemble cysts - capsules with liquid. Such a formation can be single or spread multiple times over the surface of the gland.
Benign thyroid adenoma rarely degenerates into a cancerous tumor. But the possibility of such a transition cannot be unequivocally denied. That is why patients with a neoplasm should regularly consult a doctor and undergo preventive examinations.
Diagnosis of thyroid adenoma
Almost any pathological conditions of the thyroid gland (inflammatory reactions, traumatic injuries, metabolic disorders, the appearance of tumors) are accompanied by the formation of nodular or other formations. For this reason, the main task of diagnostics can be called the differentiation of a benign process from a malignant one. Any one study will not make it possible to determine an accurate diagnosis, therefore, several studies are often prescribed based on the combined results.
- Physical examination and assessment of clinical symptoms. What should attract the doctor's attention:
- tumor growth rate;
- its consistency;
- the presence of pressure on nearby organs (respiratory tract and esophagus);
- cohesion or mobility of the formation;
- difficulty swallowing;
- hoarseness when speaking;
- condition of the cervical lymph nodes.
- Laboratory and instrumental diagnostic measures, assessment of organ performance:
- thyrotoxicosis phenomena are detected in the thyrotoxic form of the disease. Such a neoplasm in most pathological cases is benign;
- decreased thyroid function allows us to refute the presence of a malignant tumor;
- Calcitonin is a standard indicator of medullary cancer, especially if the amount of calcitonin increases within a few minutes after an intravenous injection of 0.5 mcg/kg pentagastrin;
- Thyroid hormone test therapy is sometimes used to differentiate benign from malignant processes. Under the influence of high doses of thyroid hormones, the tumor may disappear if it is benign. In other cases, surgical intervention is indicated;
- Ultrasound of thyroid adenoma helps to distinguish cysts from adenomas. In some cases, light circles or spots can be found near the tumor, which until recently was considered one of the reliable signs of a benign neoplasm. But not so long ago, this opinion was refuted. Since it is not possible to determine histological signs using ultrasound, ultrasound is considered justified only in the following situations:
- To identify multiple formations.
- For examination of a pregnant woman when isotope studies cannot be performed.
- For differential diagnosis of thyroid adenoma and cyst.
- To control the dynamics of the process.
- To facilitate aspiration biopsy of a small tumor that cannot be localized by palpation (so-called ultrasound-guided biopsy).
- Thyroid scintigraphy. This is an additional examination method that indicates the presence of cold lesions (without isotope inclusions), hot lesions (isotope inclusions are stronger than the remaining thyroid tissue), or lesions with an intermediate amount of isotope inclusions. Large malignant lesions are often cold, and benign lesions are hot.
- Computerized tomography and magnetic resonance imaging can be used to monitor the condition of tissues after tumor removal.
- The aspiration biopsy method is perhaps the main method for determining the nature of thyroid tumors:
- the cellular material is removed using a thin needle and a special syringe. Only the amount of material that is sufficient for cytology is taken. This is a fairly simple procedure, relatively inexpensive, safe and can be performed on an outpatient basis. The spread of tumor cells with the movement of the needle is excluded;
- In the case of the follicular form, in addition to a biopsy, a histological analysis of the tissues removed during surgery is required. Often, follicular tumors ultimately turn out to be papillary or follicular carcinomas (in 28% of cases), follicular adenomas (in 34% of cases), or colloid goiter (in 38% of cases).
Most neoplasms do not manifest any clinical symptoms and are detected by chance, for example, during a routine examination.
What do need to examine?
How to examine?
Who to contact?
Treatment of thyroid adenoma
Treatment with medications is based on the use of drugs that suppress the production of thyroid-stimulating hormone: such therapy is called suppressive. This type of treatment involves taking thyroxine in an amount of 2-5.2 mcg / kg of weight per day. The average daily dosage is from 150 to 200 mcg. Suppressive therapy is considered quite serious and responsible, so it is carried out only as prescribed and under the supervision of a doctor.
The possible consequences of such therapy are known: mainly, they include osteoporosis and cardiovascular disorders.
Suppressive therapy can give a positive result in approximately 80% of cases of neoplasm formed due to iodine deficiency, or in 15% of cases of the thyrotoxic form.
Against the background of drug treatment of thyroid adenoma, the use of phytotherapy is encouraged - treatment using medicinal plants. It is recommended to use plants that can inhibit the production of hormones or have a detrimental effect on the affected tissue. Such herbal remedies include blackhead, European water lily, catharanthus (pink periwinkle), colchicum, yew, etc.
Among the most effective and widespread medications are levothyroxine, L-thyroxine, propicil, microiodite, carbimazole, etc.
Suppressive treatment with levothyroxine is the most preferred form of therapy. However, it should be recognized that the suppression method does not always allow the tumor to regress completely. In addition, levothyroxine intake can often become lifelong to prevent recurrence of the tumor.
Treatment of toxic thyroid adenoma can be carried out using radioiodine therapy. In most European countries, this treatment is considered advantageous and safe; small doses can be taken even in outpatient settings. Usually, the patient is offered a preparation of radioisotopes of iodine in the form of a capsule or an aqueous solution. The essence of this method is the ability of thyroid cells to bind and accumulate the radioisotope of iodine I¹³¹, which has a damaging effect on thyroid tissue. This helps to reduce the size of the tumor and inhibit the secretion of hormones by it. The method is considered absolutely safe, although an insignificant amount of radioisotope may end up in the cells of the kidneys and intestines: this is considered an acceptable phenomenon that does not go beyond physiological limits.
Treatment of follicular adenoma of the thyroid gland is often carried out using the ethanol destruction method. This treatment is narrowly focused on tumor suppression and is based on the use of a sclerosing drug, which is injected deep into the tumor tissue. 1-8 ml of ethanol is injected directly into the tumor (depending on the size of the tumor). This procedure is repeated until the tumor is completely destroyed and stops producing hormones. Ethanol destruction can be used for small numbers and not very large tumors.
Thyroid adenoma surgery
Surgical treatment for thyroid adenoma is used in the following cases:
- if drug therapy is ineffective;
- in follicular form;
- when the tumor puts pressure on nearby tissues and organs;
- with concomitant thyrotoxicosis;
- in case of a large tumor for aesthetic reasons.
Of the many surgical interventions for thyroid adenoma, the best option is chosen, from which the best effect can be expected. Usually these are the following types of operations:
- removal of a section of one lobe;
- removal of sections of both lobes;
- hemithyroidectomy – resection of half of the gland, that is, the entire lobe with the isthmus;
- subtotal resection – almost complete removal of an organ with preservation of a small part;
- thyroidectomy – complete removal of the organ.
For a benign thyroid adenoma to require surgical intervention, it must reach a large size or cause difficulty breathing or swallowing in the patient. Surgery is also recommended in the case of active hormone production with a change in the overall level of hormones in the bloodstream.
If a patient has one benign thyroid adenoma that requires surgical intervention, then, as a rule, hemithyroidectomy is performed - removal of the thyroid lobe that contains the tumor. If the tumor is of significant size, then partial resection can only increase the risk of recurrence of the pathology. In such cases, as well as in the case of multiple tumors, complete removal of the organ is performed - thyroidectomy.
Surgery for follicular adenoma of the thyroid gland involves removing the lobe of the gland containing the tumor. The removed lobe is sent for histology after the surgery, and after 3-5 days the doctor receives an assessment of the tumor structure. If the diagnosis of "follicular adenoma" is confirmed, then no further treatment is required, and the operated patient continues to live with the remaining lobe of the thyroid gland, which usually produces enough hormones for normal functioning. If the histology shows that the follicular tumor was malignant, then a repeat operation is performed to remove the remaining lobe of the gland to prevent a relapse of oncology.
Removal of thyroid adenoma
In some cases, the doctor may prescribe additional preparation for the operation. The preparatory stage includes:
- normalization of the total amount of T3 and T4 hormones in the bloodstream. This may require increasing the dose of antithyroid drugs (propylthiouracil, mercazolil, tyrosol, etc.);
- correction of systolic and diastolic pressure, as well as cardiac activity in elderly patients;
- assessment of the patient's condition by a therapist and, if necessary, other specialists.
Before going to bed, on the eve of the surgery date, the patient is given a sedative to relieve stress and ensure a good night's sleep. In the morning, the doctor makes markings on the patient's neck to ensure a careful operation. The procedure is performed under general anesthesia, possibly with the use of endoscopic equipment. The main type of surgery involves making an incision in the thyroid gland projection area, 6 to 8 cm long. The surgeon separates the tissues and exposes the thyroid gland. After examination, he begins removing the affected area by ligating small vessels, then evaluates the surgical area and monitors its condition. If all is well, the doctor begins suturing with restoration of all neck structures. Sometimes a drain is inserted into the incision - a thin rubber or silicone tube from which interstitial fluid and blood residues can be removed immediately after the surgery. The drain is removed the following day.
Most patients are discharged from the hospital after 2-5 days. If the patient has had the entire gland removed, then immediately after the operation he is prescribed hormone replacement therapy to maintain normal hormone levels in the bloodstream. Most often, such treatment involves taking thyroxine every morning, half an hour before meals. With the correct dosage, taking the drug does not cause the development of side effects.
After 1-3 months, the wound heals completely. Already 1 month after the operation, the patient can return to his normal lifestyle.
Prevention of thyroid adenoma
Among preventive measures, lifestyle plays a major role:
- regular physical activity (aerobics, yoga, swimming pool);
- having an interesting job and a friendly team, peace and a well-established family life, no stress;
- periodic trips to the sea.
The sea is a source of relaxation and sea salt necessary for the body. If possible, it is necessary to go to the sea for health improvement at least once every two years. The rest of the time, iodized salt should be consumed (in areas poor in iodine). The diet should be reviewed:
- consume fermented milk products (kefir, cottage cheese, yogurt);
- introduce seafood and seaweed into your menu several times a week;
- eat nuts, seeds, dried fruits, citrus fruits, greens, vegetables, drink green tea with honey and rosehip infusion.
Limit the following foods in your diet: sugar and sweets, margarine, alcoholic beverages, preservatives, fast food, instant foods, croutons and chips, sauces.
To increase stress resistance, it is necessary to establish a sleep and rest regime: you should sleep for a sufficient amount of time for the body, arrange full weekends with trips to nature and active recreation.
Prognosis of thyroid adenoma
Nowadays, many specialists prefer to observe the neoplasm, postponing the operation only as a last resort. Sometimes this is justified, because the operation can entail a number of complications, for example:
- recurrent nerve palsy;
- postoperative hypoparathyroidism (disorder of the parathyroid glands);
- postoperative bleeding (in 0.2% of cases);
- subcutaneous hematoma;
- addition of purulent infection (in 0.1% of cases).
However, all possible complications are completely cured with a timely and adequate approach. The patient, preparing for surgery, should be informed about possible complications, but this should not be a reason to refuse surgery. Surgery has reached great heights in the last decade, and surgical treatment continues to be the most effective and safe. Naturally, direct indications are required for prescribing surgery, it is important to remember this.
The prognosis for thyroid adenoma is more favorable in young people than in patients over 40 years of age.
When the process becomes malignant, the prognosis becomes unfavorable, especially in the presence of metastases in the lymph nodes and organs.
Thyroid adenoma is an initially benign disease, so with timely treatment the prognosis can be favorable.