
All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Scoliosis of the thoracic spine
Medical expert of the article

Last reviewed: 12.07.2025
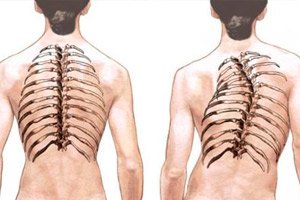
When the spine in the frontal plane deviates to the left or right with simultaneous rotation of the thoracic vertebrae, and this curvature is localized in the thoracic (thoracic) section of the spinal column, thoracic scoliosis is diagnosed. And such scoliotic deformation is the most common type of scoliosis.
Epidemiology
Congenital scoliosis is detected in one newborn out of 10 thousand [ 1 ]. With imperfect osteogenesis, the incidence of scoliosis in children ranges from 26-74.5%.
In 80-85% of cases, thoracic scoliosis is idiopathic. [ 2 ] Juvenile scoliosis develops at the age of 4-10 years and accounts for 10-15% of all idiopathic scoliosis in children. [ 3 ] The prevalence of adolescent idiopathic scoliosis, according to the Journal of Children's Orthopaedics, is 0.5%-5.2%.
According to some studies, the incidence of asymptomatic thoracic scoliosis in adults aged 25-65 years is estimated at approximately 13.4% (with a predominance of women): with a curvature angle of 10-20° – 11.6%; with a curvature of 20-30° – about 1.6%, and with a Cobb angle of more than 30° – within 0.2%. [ 4 ]
According to statistics, up to 20% of cases of left-sided thoracic scoliosis are caused by either congenital skeletal anomalies or neuromuscular pathologies. [ 5 ] This deformation can be detected at any age, but most often such scoliosis develops in adolescents (in particular, girls).
Causes thoracic scoliosis
In most cases, the causes of thoracic scoliosis (spina vertebrae thoracicae) are unknown. According to experts, its cause can only be determined in 15-20% of cases.
Thoracic scoliosis in a child may be congenital, although it is more often detected in children aged 10 to 18 years (and it affects girls to a greater extent). The congenital form of scoliosis that an infant has is the result of spinal abnormalities that develop in the fetus during pregnancy, so it is usually detected at an earlier age than idiopathic scoliosis (with an unknown etiology).
Read more in the publications:
Possible causes of thoracic scoliosis include:
- spinal or spinal cord injuries;
- infections, in particular, the poliovirus, which causes spinal paralysis in children - poliomyelitis, as well as some pathogenic bacteria that cause spondylitis;
- congenital defects, primarily spina bifida, hemivertebra, short neck syndrome, spondylothoracic dysostosis, etc.;
- osteogenesis imperfecta or hereditary skeletal dysplasia (caused by mutations in collagen genes);
- CP (cerebral palsy);
- neurofibromatosis;
- genetically determined damage to spinal motor neurons - spinal muscular dystrophy;
- syringomyelia (bone marrow damage);
- neoplasms of the spine or spinal cord (cysts, tumors).
Read also – Scoliosis: what causes it and how to recognize it?
Risk factors
Orthopedists draw patients' attention to such risk factors for the development of thoracic scoliotic curvature as:
- family predisposition; [ 6 ]
- childhood and adolescence (from 10 to 15 years), that is, the period of intensive growth in children;
- postural disorders in children, which can lead to postural scoliosis;
- increasing thoracic kyphosis in adolescents with the development of Scheuermann's disease, often accompanied by scoliotic curvature;
- different leg lengths (congenital or acquired);
- dislocations and fractures of the vertebral joints;
- formation of fibrous (scar) tissue after direct thoracic surgery;
- presence of rheumatoid arthritis;
- neuromuscular disorders; [ 7 ]
- increased doses of ionizing radiation;
- acquired or hereditary metabolic pathologies, such as mucopolysaccharidosis type IV (Morquio syndrome). See also - Some diseases accompanied by spinal deformity
- presence of a family history of scoliosis or degenerative-dystrophic diseases of the spine.
Pathogenesis
In vertebrology, the pathogenesis of thoracic scoliosis is considered taking into account the anatomical features of the thoracic - the longest section of the spine, which in the lateral projection has a natural posterior bend - kyphosis (with a curvature of 20-45 °). This physiological bend, together with the cervical and lumbar lordosis, ensures the balance of the spinal column.
The thoracic region includes the thoracic vertebrae T1–T12, as well as half of the seven dozen facet joints of the spine. In addition, there are two dozen bone-transverse joints connecting the thoracic vertebrae T1–T10 to the ribs; these joints are formed by the articulation of the transverse processes of the thoracic vertebra and the tubercle of the adjacent rib (with each rib having two articulations).
In addition, the bodies of the T1-T10 vertebrae have sides with cartilaginous depressions (for articulation with the heads of the ribs); the sides of the T2-T9 vertebrae are hemispherical; the spinous processes are long and inclined downward. The location of the ribs and spinous processes significantly limits flexion and extension of the thoracic vertebrae. The greatest rotational capacity is in the T5-T8 vertebrae.
And the fibrocartilaginous “pads” between the bones – the intervertebral discs of the thoracic spine – are the thinnest in the entire spinal column.
What happens with thoracic scoliosis? A complex deformation of the spine occurs – with lateral curvature relative to its frontal axis and a rotational component in the form of rotation (torsion) of the vertebral joints around their axes. In thoracic scoliosis in a child, the mechanism of torsion development may be due to uneven growth of the anterior and posterior parts of the vertebrae; their frontal displacement; pathological changes in the spaces between the vertebral bodies; disruption of the ossification centers on the bodies and processes of the vertebrae (which develop during puberty); insufficient mineralization of bone tissue, etc.
As the condition progresses and the vertebral bodies rotate, their height and the thickness of the intervertebral discs decrease; the vertebral bodies and spinous processes deviate toward the concave side of the scoliotic curve, and the ribs articulated with them also move in that direction, approaching each other. At the same time, on the convex side of the large curve, the ribs begin to diverge.
Symptoms thoracic scoliosis
The first signs of thoracic scoliosis begin to manifest as a violation of body symmetry, in particular, different heights of the right and left shoulder-scapular regions.
In most cases, patients with adolescent idiopathic thoracic scoliosis do not experience pain. About a quarter of patients with adolescent idiopathic scoliosis experience back pain, particularly pain in the back wall of the chest on the side of the rib protrusion. [ 8 ] Although pain in thoracic scoliosis can occur with a significant degree of curvature. More information in the material - Scoliosis as a factor in the development of back pain.
Symptoms of rotational (deforming) scoliosis of the thoracic spine include: asymmetry of the shoulders and the entire chest, the formation of a muscle roller on the back of the neck, protruding shoulder blades or ribs, a distorted waist line, and a visual shortening of one lower limb.
See also - Symptoms of Scoliosis
Stages
The degree of thoracic scoliosis is determined by X-ray: on the X-ray image of the thoracic part of the spinal column, special markings are made according to the method of the American orthopedic surgeon John Robert Cobb (1903-1967), and then the angle of curvature is measured - the Cobb angle. [ 9 ], [ 10 ], [ 11 ]
Mild curvature – thoracic scoliosis of the 1st degree – is recorded when the Cobb angle is no more than 10°.
Thoracic scoliosis of the 2nd degree is determined when the angle of curvature is 10-25°; at an angle of 25-40 (50)°, scoliosis of the thoracic spine of the 3rd degree is diagnosed, and if the angle is more than 40 (50)°, then it is scoliosis of the 4th degree.
There are three stages of the evolution of thoracic idiopathic scoliosis: the primary period of progression, the secondary period of progression, and the stable period. The chronology of these different periods is not the same. In “infantile scoliosis,” the main period of accelerated increase in the curve occurs before the age of 6. In “juvenile-pubertal scoliosis,” it occurs from the age of 6 to the first stages of puberty, and in “pubertal scoliosis,” the main increase occurs during puberty or adolescence. [ 12 ]
Forms
There are various forms, types or kinds of scoliosis of the thoracic spine, which are classified according to such parameters as anatomical features of the curvature, causes, age, etc. (therefore, there are several such classifications, which creates certain difficulties with terminology).
Left-sided thoracic scoliosis is defined as a curvature to the left: it can be congenital or secondary to various muscle and tissue disorders, such as muscular dystrophy or the growth of a spinal cord tumor.
Thoracic right-sided scoliosis or right-sided thoracic scoliosis is defined when the primary curve of curvature occurs to the right of the vertical axis of the spine and, depending on the severity, gives the spine a “C” or “S” shape.
S-shaped thoracic scoliosis has an additional curve in the opposite direction, which occurs as a result of the body's attempt to compensate for the abnormality. It is usually diagnosed in children or adolescents between the ages of 10 and 15 – during the first growth spurt; in adults, S-shaped scoliosis can be the result of various muscle or connective tissue disorders.
Idiopathic thoracic scoliosis means that the cause is unknown. It is the most common form of scoliosis in adolescents: adolescent idiopathic scoliosis affects up to four out of every 100 children over the age of ten.
Dysplastic thoracic scoliosis – with the peak of the scoliotic curvature at the T5-T9 vertebrae – develops in the presence of congenital anomalies in the formation of the structures of the thoracic spine: abnormalities in the structure of the vertebral bodies (with the development of asymmetric or wedge-shaped vertebrae), defects in their spinous processes (underdevelopment or hypertrophy), dysplasia of the intervertebral discs. Such scoliosis can be called congenital or idiopathic dysplastic, since the etiology of a significant part of the deviations in the intrauterine formation of the spine and related structures remains unknown.
Deforming scoliosis of the thoracic spine (although scoliosis itself is related to deforming dorsopathies) is defined as a structural or rotational curvature of the spinal column with morphological changes resulting in displacement of parts of the skeleton.
Scoliosis is a neuromuscular disorder, a rapidly progressing type of spinal curvature that develops with spinal cord injuries and certain neurological or muscular diseases (Duchenne muscular dystrophy, cerebral palsy, myelodysplasia).
Degenerative scoliosis, also known as adult scoliosis or de novo scoliosis, develops slowly and is a consequence of normal aging: wear and tear of the spinal joints and osteoporotic degeneration of the intervertebral discs in older people. But it most often occurs in the lumbar spine.
Complications and consequences
What is dangerous about thoracic scoliosis? This is a progressive condition, i.e. the angle of curvature increases, and over time the protrusion of the ribs leads to the formation of a rib hump.
With scoliosis of the thoracic spine of 3-4 degrees, there is a deformation of the chest, which results in compression and displacement of the organs located in the mediastinum. At the same time, the volume of the lungs decreases, which is fraught with shortness of breath, the development of pulmonary insufficiency, [ 13 ], [ 14 ] heart problems arise (with left-sided deformation of the thoracic spine). [ 15 ], [ 16 ]
There is also pinching of the intercostal and spinal nerves with intense pain – chronic neuropathic pain syndrome.
Compression of blood vessels (mammary arteries), increased blood pressure, headaches are possible.
The consequences of severe thoracic scoliosis are limited mobility and work capacity with disability.
Diagnostics thoracic scoliosis
The Scoliosis Research Society (USA) recommends annual screening for all children ages 10 to 14. The American Academy of Pediatrics has recommended screening using the forward bend test at routine health care visits at ages 10, 12, 14, and 16.
The classic screening test for scoliosis is the forward bending test, which involves the patient bending forward at the waist with the knees straight and the palms together.[ 17 ] The physician should look for any asymmetry in the contours of the back as a result of the spinal deformity in rotation.[ 18 ] In classic thoracic scoliosis, the patient's right side is prominent with a curved apex.
All types of scoliotic deformation are diagnosed in the same way, and the basis is instrumental diagnostics: radiography with spondylometry and computed tomography of the spine [ 19 ], [ 20 ]
Read also:
Differential diagnosis
Differential diagnostics are carried out. In particular, in the absence of obvious external signs of deformation, but in the presence of painful sensations in the spine and between the shoulder blades, it is necessary to differentiate scoliosis and thoracic osteochondrosis, intervertebral hernia, arthrosis or alteration of the facet joints of the thoracic spine, as well as ossification or calcification of its ligaments.
Who to contact?
Treatment thoracic scoliosis
Scoliosis takes many different forms, there is no cure for this pathology, and treatment may give temporary results, since the deformation process progresses (in 60% of rapidly growing prepubertal children).
Correction of curvature in childhood can be carried out by longitudinal stretching of the spine – traction therapy.
To stabilize the spine and reduce the load on its deformed area, rigid orthotic braces are used, as well as a fixing or corrective orthopedic corset for thoracic scoliosis (which should be worn 18 hours a day).
One method that may be useful for correcting the position of the vertebrae and increasing the stability of the spine, leading to relief of back pain soon after application, and having a positive effect on the quality of life, is kinesiotaping or taping for thoracic scoliosis (from the English taping - wrapping) - using elastic therapeutic tape (kinesio tape). [ 21 ], [ 22 ]
Patients with thoracic scoliosis place more hope in physiotherapy treatment. It should be borne in mind that massage for thoracic scoliosis will not correct the curvature of the spine: it is an auxiliary method that helps to relax asymmetrically tense paravertebral fascia and muscles, reduce chronic back pain, and improve mobility. [ 23 ]
Shiatsu is also used - a Japanese acupressure massage for thoracic scoliosis, which gently stimulates blood circulation and nutrition of limited areas of muscle tissue around the spine.
Exercise therapy for thoracic scoliosis plays a key role in long-term symptom reduction and limiting the functional impact of spinal curvature. [ 24 ] Special exercises for thoracic scoliosis, taught by exercise therapy instructors, help develop coordination and form new “muscle memory” needed to stabilize the spine and reduce curvature. [ 25 ], [ 26 ]
There are special exercises for thoracic scoliosis: according to the method of Katharina Schroth - for postural correction and correction of the scoliotic type of breathing; functional gymnastics SEAS (Scientific Exercise Approach to Scoliosis - a scientific and practical approach to scoliosis) - according to an individual program adapted to a specific patient (depending on the type and degree of scoliosis). Gymnastics is aimed at correcting the curvature and reducing the risk of increasing its arc during the growth period (in children and adolescents), and in adults - at stabilizing the curvature and reducing the level of disability. Exercises are performed two to three times a week for 45 minutes; they train the neuromotor function in order to reflexively stimulate self-correcting posture in everyday life. [ 27 ], [ 28 ]
Thus, chiropractic techniques are known to correct a curved spine, restore muscle imbalances, help restore spinal nerve function, relax muscles, and increase range of motion. [ 29 ], [ 30 ], [ 31 ]
Strengthens the muscular corset of the back and the muscles on the convex side of the spine yoga for thoracic scoliosis. Recommended hatha yoga asanas are Vashisthasana, Adho Mukha Svanasana, variations of Ardha Shalabhasana, Anantasana. [ 32 ], [ 33 ]
Swimming, which does not involve shaking of muscles and vertebral joints, helps to increase muscle strength in patients with scoliosis. In addition, water during swimming has a massaging effect on the muscles of the back, chest and shoulder girdle, improving their blood supply. How to swim with thoracic scoliosis? Vertebrologists advise avoiding strong overstrain of the back and arm muscles and recommend a style such as breaststroke. [ 34 ], [ 35 ] Although swimming is considered a complete sport and a treatment option for scoliosis, some studies contradict this approach. [ 36 ]
More information in the article: Treatment of scoliosis
When the curvature reaches 45 or 50°, osteotomy options are considered - a surgical intervention to eliminate/correct the deformity and fix the curved vertebrae. [ 37 ] The main surgical treatment is spinal fusion or spinal fusion (selective fusion of the vertebrae). [ 38 ] The vertebrae are fixed with special metal structures (which are attached to the spine with hooks or screws above and below the area of the curve) using bone autograft or allograft, which fuses with the bone tissue of the spine. [ 39 ]
As clinical experience and research results show, almost a third of patients who have undergone surgery will lose all its benefits within ten years. Every fifth patient will eventually need further operations. [ 40 ] Long-term complications of spine surgery include: postoperative coronary decompensation (4 to 41%), [ 41 ], [ 42 ] limitation of mobility (by 20-60%); damage to spinal nerves (leading to various neurological problems), chronic pain (occurring in 30% of patients operated on), permanent disability (in 40% of cases).
Read more:
Prevention
Congenital and idiopathic scoliosis of the thoracic spine cannot be prevented. The main prevention is screening: orthopedic examination of the spine in children should be carried out annually, and in 10-12 year olds - every 6-9 months.
Forecast
Doctors cannot completely correct the skeletal deformation that thoracic scoliosis causes. Its prognosis depends on the degree of curvature, its causes, the characteristics of the body and especially the musculoskeletal system of the patients, as well as the effectiveness of the treatment.