
All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Microsporidia
Medical expert of the article

Last reviewed: 06.07.2025
Microsporidia are a group of protozoan microorganisms belonging to the class of cnidosporidia. These are intracellular parasites that are unable to exist outside the host organism. There are almost 1,300 species, represented by almost 200 genera. This is only a fraction of the true diversity of mycorsporidia that has already been described in the scientific world: many possible infected hosts have not been examined for the presence of these parasites in the body. The host can be almost any animal – from protozoa to humans. The largest number and diversity of microsporidia are represented by crustaceans and insects.
Humans can become infected with microspodiaceae of six genera: Encephalitozoon, Pleistophora, Nosema, Vittaforma, Enterocytozoon, and Microsporidium. Although some parasites in this group are likely to cause asymptomatic or transient intestinal infections, the mechanism of infection with microsporidiosis has not been sufficiently studied.
Microsporidia have several unique features that demonstrate their exceptional adaptability to intracellular parasitism. Their spores contain a set of organelles that are unique to them – the extrusion apparatus. With its help, a healthy cell is infected by puncturing the membrane and releasing spores directly into the cytoplasm. No other species of protozoa have a similar mechanism for distributing their spores.
 [
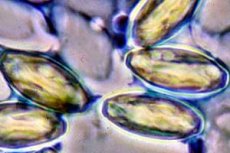
[ Structure of microsporidia
The microsporidia genome is the smallest among all cells containing a nucleus. There are almost no introns in the cells, and mitosis is presented in the form of closed intranuclear pleuromitosis. The ribosomes of microsporidia are similar in structure to the ribosomes of cells with an anuclear structure. The cell does not have kinetosomes, lysosomes, or particles of reserve nutrients. Previously, it was believed that microsporidia did not have mitochondria, but not long ago small mitosomes were found in them, which served as evidence of their mitochondrial nature.
Spores usually have a three-layer membrane: a glycoprotein exospore, a chitinous endospore, and a cytoplasmic membrane. The extrusion apparatus consists of a posterior vacuole, an anchor disk, a polaroplast, and a polar tube. The posterior vacuole has a single-chamber or multi-chamber structure. Sometimes the vacuole contains a posterosome. At the moment of the release of the embryo into a healthy cell, it immediately increases, displacing the spore into the polar tube.
The polaroplast usually consists of membranes compactly located in a kind of "package".
Sometimes the polaroplast contains vesicles and tubular structures. The polaroplast is involved in generating the necessary pressure required to evert the polar tube, provides the polar tube with a membrane and the sporoplasm making its way inside it. The polar tube is an elongated, two-membrane formation, laid out in a spiral and extending from the anchor disk. Their appearance and development can vary greatly in microsporidia.
Life cycle of microsporidia
The sporoplasm is a single nucleus surrounded by a small amount of cytoplasm containing ribosomes. The nucleus is located in the spore. Once the spore penetrates the internal environment of the host cell, the sporoplasm forms its own protective cytoplasmic membrane, about which little has yet been learned.
Then the sporoplasm grows rapidly. At this point the cell has a minimum of organelles: posterosome, ribosomes, smooth and rough endoplasmic reticulum.
With the onset of the sporogony phase – sporont – the cell acquires another membrane. In this phase, the nuclei actively divide, forming plasmodia.
Microsporidia can lay down another additional shell - a sporophore vesicle, the appearance and size of which vary significantly among different species.
Sporoblast is an intermediate stage of development from sporogonal plasmodium to spore. During this period, all membranes actively develop and organelles are laid down. Then the affected cell is destroyed, and the resulting spores attack neighboring healthy cells or are excreted from the body in search of a new host.

Microsporidia are characterized by a variety of life cycles. This cycle includes only one host (monoxenic) with the formation of one type of spores, it is typical for 80% of known species. But it can also vary greatly among different species: features of sporogony, number and types of divisions at all stages. For the remaining 20%, the life cycle can take place in two or more hosts, with the formation of different types of spores in structure and assigned functions.
Clinical picture and symptoms of microsporidiosis
Microsporidia are very common. The diseases caused by microsporidia, as well as the routes of infection, have not yet been sufficiently studied. Microsporidia, which can live in human cells, also affect animals, both wild and domestic, but it is not yet clear whether people are infected from animals. People with suppressed immunity can be carriers. Microsporidia spores are present in water bodies, but not a single case of rapid spread of the disease has proven that contaminated water is to blame. Microsporidia are excreted from the host's body into the external environment with feces, urine and sputum. It is assumed that people can become infected from each other, but there is no exact data. Most likely, intestinal microsporidiosis is contracted when the parasite enters through the oral cavity. Mainly, we are talking about an infection caused by Enterocytozoon bieneusi, which affects the gastrointestinal tract.
Microsporidiosis of the respiratory system is caused by parasites that are almost never present in feces, so the most likely way of infection is airborne dust. Eyes are affected due to the parasite getting directly into the conjunctiva. Research indicates that microsporidia can attack macrophages and fibroblasts of their own mucous membrane.
Intestinal microsporidiosis is common, but there are many variations of the disease: microsporidiosis of the bile ducts, eyes, sinuses, respiratory tract, muscle fibers, disseminated microsporidiosis, attacking the kidneys, liver, heart and nervous system.
Microsporidia, when infected, often cause acute or chronic diarrhea. Those who have undergone organ transplantation and the resulting immunodeficiency are more likely to become infected with microsporidiosis. Some cases of epilepsy are associated with the fact that the body was attacked by microsporidia. Cases of keratitis and corneal ulcers have been described that arose as a result of damage by Nosema ocularam, Vittaforma corneae and other microsporidia that have not yet been classified. Microsporidia have been detected in inflammation of muscle fibers. Nosema connori is the cause of disseminated microsporidiosis. From a quarter to a half of cases of prolonged diarrhea of unknown etiology in patients with immunodeficiency are associated with microsporidia.
Usually, parasites attack young people with lymphocytes less than 100 µl, microsoridiosis is also found in children with severe immunodeficiency. Children whose organs are affected by microsporidiosis may lag behind in development, periodically complain of abdominal pain and constant diarrhea.
Enterocytozoon bieneusi attacks intestinal cells, causing inflammation and damaging the villi, but almost never penetrates its own mucous layer. The infection is limited to the gastrointestinal tract. Encephalitozoon intestinalis, on the contrary, often develops outside the gastrointestinal tract. Getting into the bile ducts, it provokes their inflammation and non-calculous inflammation of the gallbladder. In HIV-infected people, parasites can attack the eyes, sinuses and lungs, and even develop into a disseminated form. Keratoconjunctivitis is characterized by reddening of the conjunctiva, discomfort from exposure to light, vision problems, a feeling that there is a foreign body in the eye. In addition, microsporidia can provoke the development of sinusitis with the release of mucus and pus from the nose. There are cases when the parasite gets into the lower respiratory tract; then, in the absence of signs of the disease, pneumonia or bronchitis may develop. In some cases, with immunodeficiency, disseminated microsporidiosis may develop. Which internal organs are affected depends on the type of parasite. Encephalitozoon hellem attacks the eyes, urinary tract, sinuses and respiratory organs. Encephalitozoon intestinalis develops within the gastrointestinal tract and bile ducts, there are cases when it attacks the kidneys, eyes, sinuses, lungs or bronchi. Encephalitozoon cuniculi is especially dangerous: it is capable of dissemination and can attack almost any organ.
Diseases caused by microsporidia
Various forms of infections caused by microsporidia are characterized by specific features.
- Enterocytozoonosis (microsporidia of the Enterocytozoon bieneusi species). The pathogen affects the cells of the small intestine. Macroscopic studies of changes in the intestinal mucosa cannot reveal. But under a microscope, you can see a violation of the shape of enterocytes, damage to microvilli, proliferation of crypts, and an increase in the number of lymphocytes.
Pathological cells gradually lose their villi and die, and spores are released to inhabit new healthy cells. The infection causes problems with digestion of food, carbohydrates and fats are absorbed worse. Diarrhea progresses, which lasts for weeks and can cause dehydration. Lack of appetite causes weight loss.
Most often, enterocytozoonosis occurs against the background of AIDS and develops in a disseminated form, attacking the respiratory tract and causing fever.
You can become infected by the fecal-oral route. Prevention of the disease is no different from the prevention of intestinal infections.
- Encephalitozoonoses (microsporidia of the species Encephalitozoon cuniculi and Encephalitozoon hellem). E. cunculi attack macrophages, blood and lymphatic vessels of the cells of the brain, liver, kidneys and other organs. When the cells die as a result of the infection, spores are released into the blood and lymph. The onset of encephalitozoonoses is acute, with accompanying fever and dysfunction of the affected internal organs. If the infection has attacked the brain, patients note severe headaches, irritation of the meninges or even meningeal syndrome. If the liver is affected, there are signs of hepatitis, if the kidneys - signs of nephritis.
The greatest risk of getting sick is in patients with AIDS. The source of encephalitozoonoses are animals. To avoid infection, it is necessary to carry out deratization in a timely manner and adhere to the rules of personal hygiene.
Encephalitozoon hellem in people with immunodeficiency is the culprit of keratoconjunctivitis, kidney inflammation and the development of renal failure. This parasite also develops in the respiratory organs, which is accompanied by fever, cough, difficulty breathing, signs of interstitial pneumonia. Often, several systems of internal organs are affected at the same time. The infection enters from a sick person through the respiratory organs, oral cavity or conjunctiva.
- Invasion (microsporidia of the species Trachipleistophora hominis). Affects muscle fibers, accompanied by muscle weakness, fever, keratoconjunctivitis. People and monkeys can become ill with the invasion, having become infected by contact.
- Septatosis (microsporidia of the species Septata intestinalis). Microsporidia first attack the cells of the intestinal mucosa and macrophages. Ulcers and necrosis develop in the foci of infection. Then the pathogen can develop in other organs. The main sign of infection is chronic diarrhea. It can provoke inflammation of the gallbladder and bile ducts. You can become infected from a sick person through food or water.
- Nosema (microsporidia of the Nosema connori species). This is a disseminated invasion. The main symptoms are nausea, vomiting, severe diarrhea, and respiratory failure. Studies will show the presence of Nosema connori in the muscle tissues of the heart, diaphragm, stomach, and small intestine, as well as in the walls of blood vessels in many organs, in the kidneys, liver, and lungs. Infection occurs through food.
- Nosema (microsporidia of the Nosema ocularum species) is a rare disease. The parasite lives in the cornea and provokes the development of combined inflammation of the cornea and the vascular membrane of the eyeball and even a corneal ulcer.
- The infestation (microsporidia of the species Vittaforma corneum) also affects the eyes.
- The invasion (microsporidia of the species Bruchiola vesicularum) attacks muscles and develops in people with immunodeficiency.
How to detect microsporidiosis?
Microsporidia are stained with some reagents, give a positive PAS reaction, but are often not recognized: their extremely small size (1-2 µm) and the absence of signs of an inflammatory process in adjacent tissues make it difficult to do so. Microsporidiosis is best diagnosed using an electron microscope. Modified three-color staining and PCR provide high-quality diagnostics.
Microsporidiosis can be suspected if the patient complains of chronic diarrhea, conjunctivitis, problems with the respiratory system, kidneys and liver, if the cause of these complaints has not been previously identified, and tests have not shown the presence of viruses, bacteria and other protozoa.
To verify the diagnosis, a stool smear is taken for analysis. If there is reason to suspect disseminated microsporidiosis, corneal swabs, urine sediment, and biopsies of the bladder and duodenum mucosa are taken for analysis. The smears are stained, and then it is possible to detect the spores of the pathogen, which acquire a reddish color under the action of the reagent, while most of the bacteria become green - the color of the background.
An electron microscope will detect the presence of the parasite in the tissues: spores with a characteristic polar tube are found in the cells.
Treatment
There is no proven treatment for microsporidiosis. Albendazole neutralizes E. intestinalis. Fumagillin has also been shown to be effective. Atovaquone and nitazoxanide reduce the severity of symptoms, but their effectiveness in combating the disease has not been studied. In HIV-infected individuals, the manifestations of microsporidiosis are reduced by antiretroviral therapy.
Is microsporidiosis dangerous? Microsporidia are often found in the body's tissues without showing any signs or causing any trouble. Most often, only with the progression of immunodeficiency in HIV-infected people or in organ transplant recipients does the infection become dangerous. But a person with normal immunity in most cases has nothing to worry about.