
All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Joints of the bones of the hand
Medical expert of the article

Last reviewed: 04.07.2025
The midcarpal joint (art. mediocarpea) is formed by the articular surfaces of the bones of the first and second rows of the wrist. It is a complex joint, block-shaped. Its joint space is S-shaped. The joint capsule is thin, especially on the back side, attached along the edges of the articular surfaces. The midcarpal joint is functionally connected with the radiocarpal joint.
The intercarpal joints (artt. intercarpeae) are slightly mobile, formed by adjacent carpal bones. The joint capsules are attached along the edges of the articulating surfaces. The articular cavities of the intercarpal joints communicate with the cavity of the midcarpal joint.
The midcarpal and intercarpal joints are strengthened by many ligaments. The most pronounced is the radiant carpal ligament (lig. carpii radiatum), which is a fan-shaped fibrous bundle that runs on the palmar surface from the capitate bone to the adjacent bones. The adjacent wrist bones are connected by the palmar and dorsal intercarpal ligaments (ligg. intercarpale palmaria et dorsalia). Some wrist bones are connected by intra-articular interosseous intercarpal ligaments (ligg. intercarpalia interossea).
The intercarpal joints also include the joint of the pisiform bone (art. ossis pisiformis), formed by the pisiform and triquetral bones and the strengthening of the pisometacarpal (lig. pisometacarpale) and pisiform-unate ligaments (lig. piso-hamatum). These ligaments are a continuation of the tendon of the ulnar flexor carpi muscle.
The carpometacarpal joints (artt. carpometacarpeae) are formed by the articular surfaces of the bones of the second row of the wrist and the bases of the metacarpal bones. The carpometacarpal joints (II-V metacarpal bones) are flat in shape and have a common joint space. Their joint capsule is thin, attached along the edges of the articular surfaces and is tightly stretched. The joint cavity of the carpometacarpal joints usually communicates with the joint cavities of the midcarpal and intercarpal joints. The capsule is strengthened by the dorsal and palmar carpometacarpal ligaments (ligg. carpometatacarpea dorsalia et palmaria). Mobility in the carpometacarpal joints of the II-V metacarpal bones is minimal.
The carpometacarpal joint of the thumb (art. carpometacarpea pollicis) differs from the others. It is formed by the saddle-shaped articular surface of the polygonal bone (trapezium bone) and the base of the first metacarpal bone. The carpometacarpal joint of the thumb, isolated from the other carpometacarpal joints, has great mobility. Around the frontal axis, which is not strictly transverse (at an angle to the frontal plane), the opposition of the thumb to the others (oppositio) is performed. Returning the thumb to its original position is called repositio. Around the sagittal axis, adduction and abduction of the thumb in relation to the second finger are performed. Circular motion is the result of combined movements relative to the frontal and sagittal axes.
The intercarpal joints (artt. intermetacarpeae) are formed by the adjacent lateral surfaces of the bases of the II-V metacarpal bones. The intercarpal and carpometacarpal joints have a common joint capsule. The intercarpal joints are strengthened by transversely located dorsal and palmar metacarpal ligaments (ligg. metacarpea dorsalia et palmaria), as well as interosseous metacarpal ligaments (ligg. metacarpea interossea). The interosseous metacarpal ligaments are intra-articular, they connect the surfaces of the metacarpal bones facing each other.
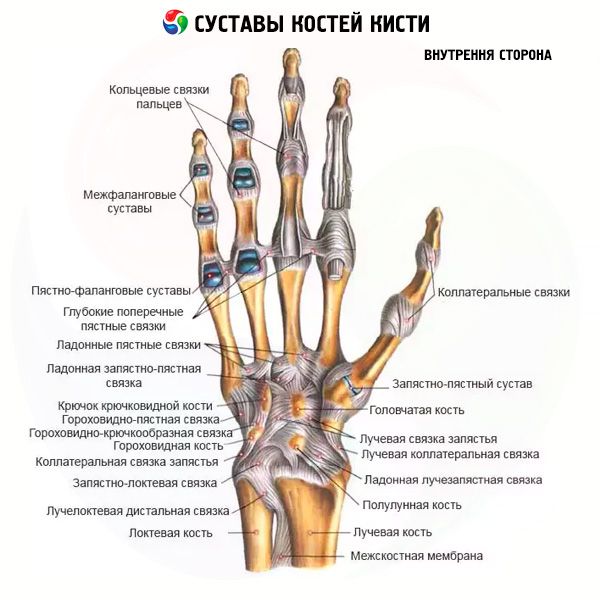
The metacarpophalangeal joints (artt. metacarpophalangeae) are formed by the bases of the proximal phalanges of the fingers and the articular surfaces of the heads of the metacarpal bones. The articular heads are rounded, the glenoid cavities on the phalanges are ellipsoid. The joint capsules are free, attached along the edges of the articular surfaces, reinforced with ligaments. On the palmar side, the capsule is thickened by the palmar ligaments (ligg. palmaria), on the sides - by the collateral ligaments (ligg. collateralia). Between the heads of the II-V metacarpal bones, deep transverse metacarpal ligaments (ligg. metacarpea transversa profunda) pass transversely.
Movements in the metacarpophalangeal joints are performed around two axes - frontal (flexion and extension) and sagittal (abduction of the finger to one side or the other).
The interphalangeal joints (artt. interphalangea) are formed by the heads and bases of the adjacent phalanges of the hand. These are block-shaped joints. The joint capsules are free and are attached to the edges of the articular cartilages. The capsules are reinforced in front and on the sides by the palmar and collateral ligaments (ligg. collateralia).
Many joints, which are called wrist joints for convenience in the clinic, participate in the movements of the hand relative to the forearm.

In the metacarpophalangeal joints, movement around two axes is possible. Around the frontal axis, flexion and extension are performed with a total volume of up to 90°. In relation to the sagittal axis, abduction and adduction are performed within limited limits. In the metacarpophalangeal joints, circular movement is possible. In the interphalangeal joints, movements (flexion and extension) are performed relative to the frontal axis. The total volume of flexion - extension in these joints is about 90°.
 [
[ Where does it hurt?
What do need to examine?
How to examine?
What tests are needed?