
All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Magnetic Calbots: A New Way to Turn Off Teeth Sensitivity
Last reviewed: 18.08.2025
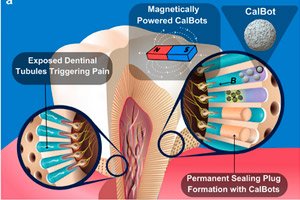 ">
">A team of materials scientists and dentists presented a magnetically sensitive bioglass nanomaterial, CalBots, at Advanced Science. This is a calcium-containing colloidal gel that, under the influence of an external magnetic field, self-organizes into short chains and penetrates deep into dentinal tubules (more than 300 microns). Inside these “microtunnels,” the material mechanically seals them and serves as a “seed” for remineralization — that is, it does exactly what most desensitizing pastes and varnishes lack: it works not on the surface, but deep down.
Background
- Where does toothache come from? When enamel wears away or gums recede, dentin is exposed - tissue penetrated by microcanals (dentinal tubules). Cold, sour, sweet or hard brushing drive fluid through these tubes to the nerve - and pain shoots through. The key to the solution is to reliably close (occlude) the tubes.
- Why conventional remedies do not work for long.
- Potassium pastes “calm the nerve” but do not close the canals.
- Fluorides, oxalates, bioglass and varnishes often form a superficial plug at the entrance, which is quickly washed away by food, acids and brushing.
- Adhesives and composites last longer, but require a dry field and often fall off over time.
- Result: there is an effect, but it is short-lived, because the blockage does not go deep.
- Why is "deep" occlusion critical? The tubes are curved and stretch for hundreds of micrometers. If the plug is only at the entrance, it is easy to destroy. If the material goes tens to hundreds of microns inside and is fixed there, it survives cleaning, acids and temperature changes much better.
- What was missing before. Even bioglass with good biocompatibility rarely reached deep: particles "got stuck" at the entrance, and without navigation they were blown away. There was no simple clinical way to deliver the material to the depths and fix it there.
- Why do dentists and patients need this? If we can standardize safe magnetic modes and confirm long-term occlusion in real conditions (acids, brush, coffee/wine), a quick office procedure will appear: apply suspension → apply magnet → get deep and stable blocking of tubes without drilling and fillings.
- What remains to be tested: Biosafety for the pulp, durability of the effect for months, reproducibility in the clinic and compatibility with other approaches (remineralization, treatment of gum recession, splints for bruxism).
Why does this even matter?
Tooth sensitivity (dentin hypersensitivity) occurs when dentin is exposed and its microscopic tubes open, through which external stimuli (cold, sour, brush) are transmitted to the nerve. Typical means (potassium pastes, fluorides, bioglasses) often give a short-term effect, because the occlusion is only maintained at the entrance to the tube and is erased by food/brushing. Therefore, now they are actively looking for ways to reliably close the tubes in depth.
What the authors came up with - in simple words
- Material: "calbots" - magnetically sensitive bioglass calcium gel. Under the right field, individual "grains" are linked into short chains (directed self-assembly). These mini-chains slide and screw into the bends of the tubes more easily than single particles.
- Delivery: An external magnet is placed on the outside of the tooth, which directs the flow of particles and helps them travel hundreds of microns through the complex “spaghetti geometry” of dentin.
- Effect: Inside the canals, the "calbots" form a plug and create a microenvironment favorable to mineralization - the key to long-term desensitization. (Bioglass is known to stimulate apatite deposition.)
What the experiments showed
- On dentine models, the authors demonstrated that the "calbots" penetrate >300 µm inside and self-assemble into structures that seal the passage of the tubes. This is as if the plug is formed not at the entrance, but inside the tube, where it is not "blown away" by a brush or acid.
- An earlier ChemRxiv paper/preprint on the same concept showed deep occlusion in human and mouse teeth and safety in animals (non-toxic up to 550 mg/kg); it also reported improvement in hypersensitivity in a controlled animal experiment. This is important context, but don't get confused: this is preclinical data from a preprint, not a clinical recommendation.
How is this different from "regular" products?
- Depth versus surface. Most desensitizers "sit" at the entrance to the tube and quickly lose their effect. Magnetically guided particles reach further and form an internal blockage.
- Navigation, not just application. Here the material is controlled: the external field sets the route and the assembly mode, so it copes better with the complex microgeometry of dentin.
What does this give to the patient (if everything is confirmed)
- Longer without "ouch!" Deep and dense occlusion should withstand food, drinks and cleaning longer - which means it will be less likely to be "punched" by cold/sour. This is still a hypothesis, but it is consistent with the fact that the longevity of treatment depends on the strength of the occlusion in depth.
- Mini-procedure in the office. In theory, this could be a short procedure at the dentist: apply a suspension, apply a magnet, check. Without removing enamel, without injections - and without daily "smearing". (The format of the actual procedure has yet to be determined.)
Where is caution?
- These are laboratory and preclinical data; there are no clinical RCTs on humans yet. Ahead: safety for the pulp, occlusion stability under real conditions (acids, brush, temperature changes), standardization of magnetic modes and reproducibility in practice.
- It is possible that patients with extensive erosion or gum problems will require a combined approach (hygiene, bruxism splints, remineralizing agents). This is recalled by modern reviews on sensitivity.
Context: Why Bioglass?
Bioglass is a favorite of dentistry: it is biocompatible, releases ions that stimulate remineralization, and is often used as a component of pastes/varnishes to seal tubes. But without active delivery, the effect quickly “washes off.” “Calbots” take the best of bioglass and add controlled navigation plus self-assembly to the “anchor” structures.
Conclusion
Advanced Science describes a clever way to deliver the material to its target — deep inside the dentinal tubules — and there it self-organizes into a stable “plug.” If subsequent clinical studies confirm its safety and durability, dentists will have a tool that works where it hurts, not just on the surface.