
All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
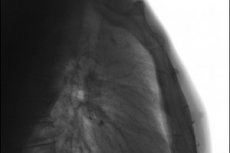
X-ray of the sternum in 2 projections
Medical expert of the article

Last reviewed: 04.07.2025
Typically, a chest X-ray is performed for diagnostic purposes, but targeted visualization of the flat breastbone in the middle of its anterior wall - a sternal X-ray - may be required.
Indications for the procedure
Indications for sternal radiography include:
- fracture of the sternum associated with injuries, including intense compression of the chest during cardiopulmonary resuscitation;
- postoperative divergence (non-union) of the sternum - after sternotomy during coronary artery bypass grafting;
- chest deformities – funnel chest, cleft sternum, Poland syndrome;
- developmental anomaly in the form of the absence of the lower part of the sternum (xiphoid process) – axiphoidia;
- anterior chest wall syndrome - costosternal syndrome (inflammation of the costosternal joints);
- suspected chondro- or osteosarcoma of the sternum.
What does an X-ray of the sternum show? On an X-ray, the sternum (sternum) – the manubrium (manubrium sterni) starting below the jugular notch, the body (corpus sterni) and the xiphoid process (processus xiphoideus) – are visible along the spine without overlapping the vertebrae, and the cortical contours of the bone are also visible above the shadow of the heart; the sternoclavicular joints (articulatio sternoclavicularis) are also visualized.
Preparation
Preparation, as with any X-ray of bone structures, is limited to the patient removing all metal-containing accessories – wherever they may be. [ 1 ]
The positioning or laying of the patient during an X-ray of the sternum is done according to the Atlas of X-ray positions and depends on the X-ray positioning, that is, on the projection in which the image of this bone needs to be taken.
Technique sternum X-rays
According to the standard, an X-ray of the sternum is taken in 2 projections: lateral (side) and anterior oblique.
A lateral sternum X-ray is the most informative in cases of sternum fracture and determining the degree of displacement, as well as identifying metastases. It is performed with the patient in an upright position (sitting or standing). In this case, one side of the patient's chest should be adjacent to the X-ray cassette, his arms are placed behind his back, moving his shoulders back (so that the chest moves forward), and the chin is raised. On command from the radiologist, the patient should hold his breath for a few seconds.
If the patient is unable to take this position due to severe pain, a parallel thin beam of radiation (collimation) is used, which allows obtaining a satisfactory image. In case of severe injuries, the procedure is performed lying down - on the side or on the back, changing the focus of the X-ray beam accordingly.
Often the lateral projection is supplemented by a right anterior oblique projection, in which the patient leans forward by 15-25°, and the central beam is directed perpendicular to the film - slightly to the left of the spinal column, in the middle between the jugular notch and the xiphoid process. In the presence of severe trauma, the X-ray is taken lying down - in the left posterior oblique projection.
X-ray signs of a sternum fracture
Chest radiographs are usually the initial imaging in patients with suspected sternal injuries. An anteroposterior radiograph has been shown to have only a 50% sensitivity for detecting sternal fractures. A lateral radiograph increases sensitivity and is usually diagnostic because most sternal fractures are transverse and any displacement occurs in the sagittal plane.
And their X-ray sign is the appearance of dark spaces on the light background of the flat sternum, which is a reflection of the fracture lines. A convincing confirmation of the fracture is the displacement of the fragments visible on the image. [ 2 ]
Today, CT is the preferred imaging method for suspected sternal fractures, as it can show possible substernal hematomas and soft tissue edema in addition to demonstrating bone integrity.
Deformation of the sternum on x-ray
In case of funnel chest deformity (Pectus excavatum), the lateral X-ray shows penetration (deflection) of the sternum into the mediastinum; often there is an anterior deflection of the thoracic spine (kyphosis), torsion of the sternum in the axial plane and a noticeable increase in its thickness.
In addition, the condition of the mediastinal organs, bones and connective tissues of the chest is assessed using ultrasound and computed tomography.
The radiographic signs of pectus carinatum include chondrogladiolar or chondromanubrial protrusion of the sternum. In the first case, its middle and lower parts protrude forward, in the second, the manubrium of the sternum protrudes (known as Currarino-Silverman syndrome).
In patients with Poland syndrome grade II, the deformation of the sternum is visible on the X-ray as a slight lateral rotation, which is much more pronounced in grade IV deformation.
X-ray signs of sarcoma of the sternum
On X-ray, osteosarcoma of the sternum appears as a formation with irregular edges and no clear boundaries, consisting of bone and soft tissue with areas of osteolytic destruction (destruction of the medullary and cortical layers of bone tissue), calcification (calcification zones), and the inclusion of osteoid matrix (non-mineralized proteins secreted by osteoblasts).
Lateral projection images can show the result of the tumor periosteal reaction – mineralization of the chondroid matrix (periosteum) in the form of bone protrusions (which specialists call spicules).
In terms of their location, pattern of bone destruction, matrix mineralization, periosteal reaction, and associated soft tissue component. However, in the evaluation of flat bone tumors, especially of the sternum, radiography has limitations: the lesion may not be fully projected due to overlapping of surrounding lung. Lateral radiographs may be helpful, especially in distinguishing intra- and extrathoracic lesions. Plain radiography has limited use in the diagnosis of small lesions and in assessing intrathoracic extension, necessitating the use of cross-sectional images.[ 3 ]
And the method of choice for instrumental diagnostics of sternum lesions is computed tomography (CT). And for local determination of the stage of sternum sarcoma (assessment of its intraosseous spread and soft tissue lesions), MRI is used.
Contraindications to the procedure
Radiography is contraindicated in severe patient conditions, during the acute phase of infectious diseases and internal bleeding, and for pregnant and breastfeeding women.
For children under 15 years of age, X-rays should, if possible, be replaced by ultrasonography (ultrasound) or MRI.