
All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Ptosis in children
Medical expert of the article

Last reviewed: 07.07.2025
Congenital ptosis
- Dystrophic - simple congenital ptosis:
- the most common anomaly of the eyelid;
- caused by dystrophy of the levator of the upper eyelid;
- increase in the latency period of the upper eyelid reaction when looking downward;
- the degree of smoothness of the fold of the upper eyelid can vary;
- accompanied by weakness of the superior rectus muscle;
- associated with blepharophimosis syndrome.
- Non-dystrophic origin:
- there is no delay in the reaction of the upper eyelid to downward gaze;
- the function of the levator of the upper eyelid is not impaired.

Unilateral congenital ptosis

Blepharophimosis Syndrome. Bilateral Operated Ptosis, Telecanthus and Blepharophimosis
- Congenital neurogenic ptosis:
- usually caused by paresis of the third pair of cranial nerves;
- distorted regeneration - ptosis may decrease with adduction, downward or upward gaze;
- cyclic paresis of the third pair of cranial nerves;
- paresis of the upper eyelid is characteristic;
- in the "spastic phase" the eyelid rises, the pupil diameter decreases, the eye assumes an adduction position;
- A “spastic phase” occurs periodically, usually lasting less than a minute.
- 4. Marcus Gunn phenomenon - palpebromandibular synkinesis:
- usually combined with ptosis;
- the eyelids rise when the patient opens the mouth, moves the lower jaw to the opposite side, or swallows;
- the phenomenon is caused by pterygoid synkinesis/
 [
[ Acquired ptosis
I. Aponeurosis defect:
- blepharochalasis;
- recurrent eyelid edema;
- acquired aponeurosis defect;
- well-defined fold of the upper eyelid;
- often has a bilateral character.
II. Neurogenic:
- paresis of the third pair of cranial nerves;
- Horner's syndrome:
- mild ptosis;
- lower eyelid lift;
- miosis;
- ipsilateral anhidrosis;
- congenital Horner syndrome:
- may be caused by birth trauma, usually due to the use of forceps during childbirth;
- usually has an idiopathic origin;
- Acquired Horner's syndrome - usually a sign of sympathetic nervous system involvement; often occurs as a consequence of thoracic surgery, including removal of chest tumors, as well as neuroblastoma that developed in infancy.
III. Myogenic ptosis:
- myasthenia gravis:
- in most cases, asymmetrical disorder;
- may be of congenital origin if the child's mother suffers from the same pathology; in this case, a transient nature is possible;
- sometimes occurs in infancy;
- accompanies hypoplasia and tumors of the thymus;
- combined with pathology of the external muscles of the eye, accompanied by double vision;
- Concomitant weakness of the orbicularis muscle is often noted;
- The Tensilon test (test using endrophonium) has diagnostic value;
- progressive external ophthalmoplegia, usually occurs in older children;
- mechanical ptosis in case of eyelid tumors, scarring, etc.

External ophthalmoplegia. Bilateral ptosis. The patient opens the eyes by raising the eyebrows.
IV. Pseudoptosis:
- disorder of upward eye movement - the fellow eye and its upper eyelid move upward, and the affected eye and its upper eyelid are unable to perform a similar movement;
- blepharochalasis with flaccid, stretched skin of the upper eyelid, which is more often observed in old age or with hemangioma of the upper eyelid.
What's bothering you?
What do need to examine?
How to examine?
Treatment of ptosis
- A complete examination of the visual organ, examination of the eyelids, including their mobility, is mandatory. The position of the eyeball is determined, the function of the oculomotor system is examined, and the presence of the Bell phenomenon is clarified.
- Treatment is usually surgical. The indication for surgery is a functional or cosmetic defect. In case of mild ptosis, surgery is performed using the Fasanella-Servat method, fixing and excising the upper edge of the cartilage and the lower portion of the Müller muscle.
- In case of congenital moderate ptosis, preference is given to one of the methods of levator resection. The cosmetic effect is better when approaching from the conjunctiva, but the anterior approach is technically simpler and allows for a larger resection. A complication of extensive levator resection is disruption of synchronous eyelid movements in both eyes when looking down and incomplete closure of the palpebral fissure at night.
- Surgical intervention for severe ptosis usually involves suturing the muscle using autogenous fascia lata or synthetic materials.
- Concomitant strabismus, especially in the presence of a vertical component, is an indication for its surgical correction.
- The results of surgical treatment of myogenic ptosis are usually unsatisfactory, there is an increased risk of such a complication as non-closure of the palpebral fissure, especially in cases of pathological Bell's phenomenon.
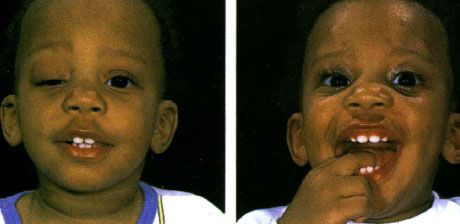
A) Severe unilateral ptosis with no upper eyelid fold on the right eye. After birth, the child was immediately prescribed occlusions of the left eye, thanks to which the visual acuity of the right eye is not reduced, b) The same child after the operation of levator suturing on both eyes. In the forehead and eyebrow area, traces of the skin from the surgical intervention are determined
Tensilon test
It is performed in older children according to the following recommendations. For young children, the dose is reduced according to their age.
- The study is carried out only if it is possible to provide cardiopulmonary rehabilitation.
- If ptosis is present, the condition of the upper eyelid and the movements of the eyeball are examined and its position is determined.
- 2 mg Tensilon (endrophonium hydrochloride) is administered intravenously and a 5-minute pause is made, waiting for the appearance of a possible pathological reaction, a decrease in ptosis or restoration of eye movements.
- After a 5-minute break, an additional 8 mg of the drug is administered intravenously for 1-2 seconds.
- The disappearance of ptosis, restoration of the correct position of the eyeball or normalization of eye movements are regarded as a positive reaction.
- The side effect in the form of a vascular reaction of parasympathetic origin can be prevented or stopped by intramuscular or intravenous administration of atropine.