
All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Prostate biopsy for prostate cancer
Medical expert of the article

Last reviewed: 07.07.2025
Before the advent of the PSA determination method, prostate biopsy was performed only to clarify the diagnosis and prescribe hormonal therapy in the case of palpable changes in the gland or metastases of prostate cancer.
Currently, early diagnosis allows for the detection of localized forms of prostate cancer and radical treatment, so biopsy is expected to provide additional information that influences the choice of treatment method.
Types of Prostate Biopsy
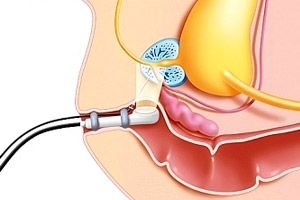
The main method of performing a biopsy is multiple puncture biopsy of the prostate gland under transrectal ultrasound control with an 18 G needle. With concomitant antibacterial therapy, the risk of complications is low. Performing a biopsy with a 14 G needle is fraught with a high risk of infectious complications and bleeding.
About 18% of prostate cancers are diagnosed when a palpable prostate mass is detected. In 13-30% of cases, the PSA level is 1 to 4 ng/ml. When a node in the gland is palpated, targeted biopsy is recommended. The sensitivity of a biopsy performed under the control of duplex ultrasound with contrast is not inferior to the sensitivity of multiple biopsy. However, this research method has not yet received general recognition.
According to research, with a PSA content of about 4-10 ng / ml, cancer is confirmed in only 5.5% of cases. With a simultaneous primary biopsy, this figure increases to 20-30. A relative indication for biopsy is a decrease in the threshold PSA level to 2.5 ng / ml. During a sextant biopsy with a PSA level of 2.5-4 ng / ml, prostate cancer detection is 2-4%, but with an extended biopsy technique (12-14 pricks) it increases to 22-27%. It should be noted that latent cancer is detected in 20% of cases (tumor volume less than 0.2 cm 3 ). Thus, a decrease in the upper limit of the PSA norm leads to the detection of clinically insignificant tumors that would not be life-threatening even without treatment. There is insufficient data yet to establish the upper limit of the PSA norm, which allows detecting non-palpable but clinically significant tumors. When determining relative readings, it is necessary to take into account other PSA indicators (increase, doubling time, etc.). Increasing the upper limit of PSA, at which a biopsy is necessary, is irrational, since there remains a high probability of detecting prostate cancer. Only at the age of over 75 years is it possible to increase the upper threshold value to 6.5 ng/ml.
Targeted prostate biopsy is necessary only in case of a palpable tumor and PSA level over 10 ng/ml. In order to clarify the diagnosis in case of metastatic or locally advanced process, it is enough to obtain 4-6 biopsies. In other cases, multiple biopsies are recommended.
In the last 15 years, the biopsy technique proposed by K.K. Hodge et al. (1989) has become widespread. Its essence is in taking biopsy samples at the midpoint between the median groove and the lateral border of the prostate gland from the base, middle part and apices of both lobes, which is why the technique was called sectant (6-point) biopsy. The 6-point biopsy method was later improved so that the posterolateral parts of the peripheral zone of the gland, which are inaccessible with the standard technique, were included in the biopsy samples. In addition, with an increase in the volume of the prostate gland, the frequency of cancer detection using the sectant technique decreases. The required number of tissue samples requires clarification. In almost all studies, an increase in the number of biopsy samples increased the sensitivity of the method (compared to a 6-point biopsy). The sensitivity of the biopsy is higher, the greater the number of biopsy samples examined. In tests on gland models it was found that if the tumor volume is 2.5, 5 or 20% of the gland volume, then with a sectorial biopsy the tumor is diagnosed in 36, 44 and 100% of cases. When performing a biopsy, it should be taken into account that in 80% of cases the tumor occurs in the peripheral zone. According to one study, taking 13-18 biopsies increased the sensitivity of the method by 35%. Vienna normograms (2003) reflect the relationship between the number of injections, the patient's age and the volume of the prostate. The accuracy of the forecast is 90%.
Dependence of the number of biopsies on the patient's age and prostate volume with a positive predictive accuracy of 90%
Age, years |
Prostate volume, ml |
|||
<50 |
50-60 |
70 |
>70 |
|
20-29 |
6 |
8 |
8 |
8 |
30-39 |
6 |
8 |
10 |
12 |
40-49 |
8 |
10 |
12 |
14 |
50-59 |
10 |
12 |
14 |
16 |
69 |
12 |
14 |
16 |
- |
>70 |
14 |
16 |
18 |
- |
It has been proven that it is inappropriate to capture the transition zone of the gland during the primary biopsy, since cancer is very rare there (less than 2% of cases). Currently, the most common is a 12-point biopsy. Great importance is attached not only to the number of punctures, but also to the angle of the needle.
Prostate Cancer Biopsy Conclusion
The histological report must necessarily reflect the following points:
- localization of biopsies; especially important when planning radical prostatectomy; the spread of the tumor to one or both lobes is taken into account when performing nerve-sparing surgery; if the apex of the gland is affected, the stage of its mobilization is more complicated; there is a high probability of a positive surgical margin when isolating the urethral sphincter;
- orientation of the biopsy in relation to the capsule of the gland; for clarification, the distal (rectal) section is stained with a special solution;
- availability of PIN;
- volume of biopsy lesion and number of positive punctures;
- Gleason differentiation of tumor cells;
- extracapsular extension - detection in biopsies of the prostate capsule, adjacent fatty tissue and invading tumor tissue, which is important for choosing a treatment method;
- perineural invasion, indicating tumor spread beyond the prostate gland with a probability of 96%;
- vascular invasion;
- other histological changes (inflammation, hyperplasia of the prostate gland).
If the above indicators are not reflected in the histological report, then it is necessary to indicate the location and number of positive biopsies, as well as the degree of differentiation of the tumor according to Gleason.
 [ 7 ]
[ 7 ]
Interpretation of biopsy data in prostate cancer
Interpretation of biopsy data requires an individual approach. If the first biopsy is negative, a repeat biopsy is necessary, the probability of detecting cancer is 10-35%. In severe dysplasia, the probability of detecting cancer reaches 50-100%. In this case, a repeat biopsy is mandatory in the next 3-6 months. It has been proven that two biopsies can detect most clinically significant tumors. Even after taking a large number of biopsies and a negative result of the first biopsy, a repeat biopsy quite often detects cancer. If prostate cancer is suspected, none of the diagnostic methods provides sufficient sensitivity to avoid a repeat biopsy. Cases of detection of a single lesion require special attention. Clinically insignificant cancer (tumor volume less than 0.5 cm 3 ) after radical prostatectomy is observed in 6-41% of cases. In this situation, it is necessary to comprehensively assess the clinical situation and determine the treatment tactics. The most important factors are the patient's age, PSA level, tumor differentiation degree, volume of biopsy lesions, and clinical stage. The presence of high-grade prostatic intraepithelial neoplasia (PIN) in biopsy samples may indicate a malignant process in the prostate gland. Such patients are recommended to undergo a repeat biopsy in 3-12 months, especially if 6 biopsy samples were initially obtained. Indications for a repeat biopsy are a palpable mass in the prostate gland, an increase in the PSA level, and severe dysplasia in the first biopsy.
Who to contact?