
All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Palpation of the liver and gallbladder
Medical expert of the article

Last reviewed: 04.07.2025
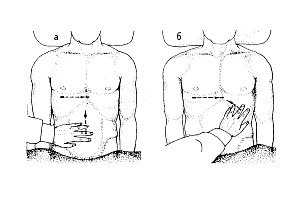 ">
">Palpation of the liver plays a major role in the physical examination of this organ. Palpation of the liver is performed according to all the rules of deep sliding palpation according to Obraztsov. The doctor is positioned on the right side of the patient lying on his back with his arms extended along the body. A necessary condition is the maximum relaxation of the muscles of the abdominal wall of the patient during his deep breathing. It is recommended to use the pressure of the palm of the doctor's left hand, located on the anterior chest wall on the right below, for a greater excursion of the liver. The palpating right hand lies flat on the anterior abdominal wall below the edge of the liver, determined by percussion, while the fingertips are located along the supposed lower edge, immersed in depth synchronously with the patient's breathing and with the next deep inhalation meet the descending edge of the liver, from under which they slip out.
When palpating the liver, its lower edge is assessed first - shape, density, presence of irregularities, sensitivity. These properties can be extended to the entire mass of the liver. The edge of a normal liver is soft when palpated, smooth, thin, painless.

The displacement of the lower edge of the liver may be associated with the prolapse of the organ without its enlargement: in this case, the upper border of the liver dullness will also be lowered. Of greater importance is, naturally, the statement of liver enlargement (hepatomegaly), which is most often observed in congestive heart failure, acute and chronic hepatitis, and liver cirrhosis. Usually, the edge of the congestive liver is more rounded and painful on palpation, while the edge of the cirrhotically altered organ is denser and uneven. Pressing on the enlarged congestive liver causes swelling of the right jugular vein - a simple but very important sign of detecting blood stagnation in the systemic circulation (reflux symptom, or hepatojugular reflux).
It should be noted that with large ascites, conventional percussion and palpation of the liver are difficult, so the method of balloting palpation (the “floating ice floe” symptom) is used, with the help of which one can get an idea of the features of the edge of the liver and its surface.
The dynamics of changes in liver size are very important. Rapid enlargement is usually observed in liver cancer, rapid reduction - in liver cirrhosis and acute hepatitis of fulminant course, as well as in successful treatment of congestive heart failure.
Hepatomegaly (liver enlargement) is a significant sign of liver damage (hepatitis, liver cirrhosis, and primary cancer or cirrhosis - liver cancer). Other causes of hepatomegaly include congestive heart failure, metastases of various tumors, polycystic disease, lymphomas (primarily lymphogranulomatosis ).
Causes of hepatomegaly
Venous congestion in the liver:
- Congestive heart failure.
- Constrictive pericarditis.
- Tricuspid valve insufficiency.
- Hepatic vein obstruction (Budd-Chiari syndrome).
Infection:
- Viral hepatitis (A, B, C, D, E) and liver cirrhosis (B, C, D).
- Leptospirosis.
- Liver abscess:
- amebic;
- pyogenic.
- Other infections (tuberculosis, brucellosisschistosomiasis, syphilis, echinococcosis, actinomycosis, etc.).
Hepatomegaly not associated with infection:
- Hepatitis and cirrhosis of the liver of non-viral etiology:
- alcohol;
- medicinal products:
- toxins;
- autoimmune disorders;
- non-specific reactive hepatitis.
- Infiltrative processes:
- fatty liver, lipoidosis (Gaucher disease);
- amyloidosis;
- hemochromatosis;
- Wilson-Konovalov disease;
- α1-antitrypsin deficiency;
- glycogenoses;
- granulomatosis (sarcoidosis).
Bile duct obstruction:
- Stones.
- Strictures of the common bile duct.
- Tumors of the pancreas, ampulla of Vater, bile ducts, pancreatitis.
- Compression of the ducts by enlarged lymph nodes.
- Sclerosing cholangitis (primary, secondary).
Tumors:
- Hepatocellular carcinoma, cholangiocarcinoma.
- Metastases of tumors to the liver.
- Leukemia, lymphoma.
Cysts (polycystic).
In addition to the above reasons, liver enlargement is observed with fatty degeneration (often of alcoholic or diabetic origin), amyloidosis (especially secondary), alveolar echinococcosis of the liver, and with large cysts and abscesses located close to the anterior surface of the organ.
Since hepatomegaly is often accompanied by an enlarged spleen (splenomegaly), it is appropriate to use the term “ hepatosplenic syndrome.”
 [
[ Causes of hepatosplenic syndrome
Diseases |
Reasons |
Cirrhosis. |
Viral infection; autoimmune disorders; primary sclerosing cholangitis, copper and iron metabolism disorders; less commonly, alcoholic, primary biliary cirrhosis. |
Granulomatosis. |
Sarcoidosis; berylliosis; histoplasmosis; schistosomiasis. |
Hemoblastoses: |
|
Myeloproliferative diseases. |
True polycythemia (erythremia); myelofibrosis; chronic myelogenous leukemia; |
Lymphoproliferative diseases. |
Chronic lymphocytic leukemia; lymphoma; lymphogranulomatosis; |
Amyloidosis. |
Waldenstrom's macroglobulinemia. |
Gaucher disease. |
|
The gallbladder becomes accessible for palpation when it is significantly enlarged: with empyema (purulent inflammation), dropsy, chronic cholecystitis, cancer. In these cases, it can be felt as a saccular body of dense or elastic consistency in the area between the lower edge of the liver and the edge of the right rectus abdominis muscle. Courvoisier's symptom is distinguished - a bladder stretched with bile with normal elastic walls (with blockage of the common bile duct by a tumor of the head of the pancreas). Very rarely, it is possible to obtain a sensation of vibration by palpation, which is transmitted to adjacent spread fingers of the left hand when tapping on one of them.