
All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Deep bite in adults and children
Medical expert of the article

Last reviewed: 04.07.2025
A beautiful, even row of teeth is not only a guarantee of an attractive smile, but also one of the conditions for the normal functioning of the digestive, respiratory and even cardiovascular systems. Unfortunately, people often do not attach much importance to the disorder of the dentition, since it usually does not cause pain, and may be barely noticeable from the outside. But in reality, the problem exists. For example, a deep bite associated with improper closure of the teeth can negatively affect the function of chewing, speech, lead to increased abrasion of the enamel coating, etc. At some degrees of such a disorder, treatment should be mandatory.
Why is a deep bite dangerous?
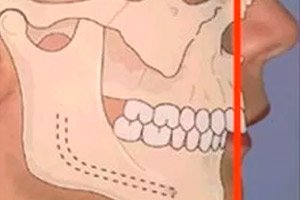
When speaking about deep bite, dentists mean a vertical occlusion defect, which is accompanied by an increased overlap of the lower incisors by the upper ones by more than 1/3 of the height. With deep bite, the appearance of the face suffers, the chewing process is difficult, speech disorders appear. Regular damage to the soft tissues of the gums and palate, increased abrasion of tooth enamel, and disruption of jaw functions are possible.
Correction of deep bite is a long, difficult process that requires a fairly large investment of both money and time. The duration of treatment varies, but the sooner the patient seeks help, the sooner he will be able to eliminate the problem. In addition, the duration of the treatment period depends on the degree of pathology, the presence of additional deformations and diseases. In any case, the doctor will be able to competently plan the treatment process, and over time, functional and aesthetic disorders will be eliminated.
If you do not begin to correct a deep bite, then periodontal diseases and diseases of the entire jaw system may develop in the future, and premature tooth loss occurs.
Epidemiology
According to statistics, about 80% of the world's population has problems with their bite. And about every third case requires specialized orthodontic treatment.
The frequency of such pathologies increases annually. Doctors explain this by the peculiarities of modern food. More and more people prefer to eat soft foods, but dense, hard food is necessary for the health of the masticatory apparatus - in particular, raw plant products. As a result, the masticatory mechanism does not receive the load it needs, and the jaws develop incorrectly.
Dentists consider deep bite to be one of the most common bite defects that patients seek medical help for. According to statistics, the population frequency of this disorder is estimated at 6-51%. Among all occlusion defects, deep bite occurs in 20% of cases. [ 1 ], [ 2 ], [ 3 ]
Doctors call this pathology “traumatic bite”, “deep incisor or frontal overlap”, “deep incisor occlusion or disocclusion”.
Causes overbite
Why does deep bite occur? Dentists have identified a number of possible causes:
- hereditary predisposition;
- pathological overload of the jaw-muscle mechanism associated with various diseases and conditions;
- early loss of baby teeth;
- abnormal growth of wisdom teeth;
- general health problems;
- developmental anomalies, presence of “extra” teeth.
All processes occurring in the body are predetermined by the human genotype, therefore genetics largely determines the structure of the maxillofacial system. Often the same problem with the bite is passed on to subsequent generations, and here the fault lies with hereditary predisposition. [ 4 ]
As for overloads or incorrect loads on the jaw-muscle system, several causal mechanisms are at work here. Firstly, most people prefer soft food to rough. Secondly, few of us have thought about the principle by which teeth are divided into different functional categories: we are talking about incisors, canines, premolars and molars.
- Incisors are designed for biting. At the moment of "biting" the necessary load is applied along the tooth axis.
- The purpose of canines and premolars is to tear and chew food, crush pieces into smaller fractions. At this time, there is a vertical load with a small horizontal force vector.
- Molars are tools for grinding food, which occurs when the lower jaw slides to the sides. During grinding, horizontal loads are present with a direction across the longitudinal axis of the teeth.
If a person has bad habits that disrupt the mechanism of the teeth, then sooner or later this leads to the development of certain dental defects.
Another indirect cause of deep bite formation is impaired nasal breathing, with predominant breathing through the mouth. How does pathology appear? The fact is that in such a situation, adequate pressure between the nasal and oral cavities is disrupted. In addition, with a systematically open mouth, the tongue takes a somewhat unnatural position, exerting excessive pressure on the lower jaw (while the upper one “rests”). [ 5 ]
Incorrect work and position of the tongue can not only cause dental and jaw disorders, but also reduce the effectiveness of deep bite treatment. Here are the factors that influence the occurrence of the disorder:
- prolonged breastfeeding;
- long-term use of nipples, pacifiers, and sippy cups;
- eating food with large amounts of liquid, the habit of drinking with food;
- shortened frenulum of the tongue.
Another negative childhood habit is thumb sucking: during this process, the upper row of teeth is pushed forward, and the lower jaw is pulled back. This is what causes the problem.
A common mistake of many adults is insufficient attention to the baby's temporary teeth. Some parents think that if the teeth will change anyway, then there is no need to pay attention to them. However, displacement often occurs precisely during this period, due to early destruction or removal of baby teeth.
Systemic diseases are another factor that adversely affects the entire body, including the dental system. Metabolic processes are disrupted, a deficiency of vitamins and microelements develops, which over time negatively affects the condition of bones and muscles.
Risk factors
The appearance of a deep bite usually occurs under the influence of various general and local factors.
The most common factors are considered to be:
- genetics, unfavorable heredity;
- dental diseases;
- maternal diseases during pregnancy (infectious and inflammatory pathologies, metabolic disorders, polyhydramnios, hypoxia, etc.);
- improper and inadequate nutrition;
- systemic disorders in the body, chronic diseases of the thyroid gland, upper respiratory system, digestive organs;
- bad habits;
- congenital defects of the maxillofacial system;
- deformation of bones and spine.
Pathogenesis
The main mechanism of deep bite formation in humans is based on the disruption of the normal physiology of the maxillofacial system. When the front row of teeth is deprived of the opportunity to experience the necessary chewing loads, it loses its correct position, rushing towards the least resistance. Such a shift is a slow process, but it occurs until the lower incisors abut, for example, against the soft tissues of the hard palate. In such a situation, traumatic occlusion can develop, in which constant traumatization of the palate is observed.
Among the causes that cause load imbalance in the anterior region of the dentition, the following can be noted:
- too long a period of breastfeeding;
- prolonged use of pacifiers and bottle nipples;
- lack of solid food in the diet;
- labial or lingual parafunction, etc.
Deep bite is classified as a vertical bite pathology. It can be formed due to genetic, intrauterine, postnatal reasons, including systemic diseases, dental and maxillofacial disorders, bad habits.
Symptoms overbite
A person can detect the first signs of a disorder and the formation of a deep bite on their own, or they can be diagnosed by a dentist during a routine appointment. The following are considered characteristic symptoms:
- the lower segment of the face is somewhat shortened, which looks disproportionate;
- the upper lip can be pushed forward, and the lower lip can be beveled or slightly tucked under the upper lip;
- thinning of the lips occurs;
- if the rows of teeth overlap significantly, the marginal gum line may be damaged;
- a person experiences discomfort when biting and/or chewing food;
- the chewing process may be accompanied by unaesthetic sounds (chomping, etc.);
- many patients experience increased enamel wear and periodontal disease;
- Speech is impaired, and it is difficult for a person to pronounce individual letters.
Deep bite in adults attracts attention with various aesthetic and functional disorders. External signs are facial and oral. Facial symptoms include shortening of the lower segment of the face, strengthening of the supramental fold, and external protrusion of the lower lip. Sometimes this type of face is called "like a bird's". Among the oral signs are the following: the lower frontal row overlaps the upper, the depth of the oral vestibule decreases, the upper jaw dominates the lower. With a pronounced deep bite, the patient can often develop stomatitis, gingivitis, periodontitis, etc.
The disorder is often accompanied by a weakening of the tone of the masticatory muscles, which leads to dysfunction and arthrosis of the jaw system. The patient experiences aching pain, discomfort and crunching in the joints, headaches. [ 6 ]
Deep bite in children, unfortunately, is often ignored. But it is in childhood that such a violation can be corrected much easier and faster. In general, doctors define the following main stages of development that affect the formation of bite features:
- period from newborn to six months of age;
- from six months to three years (during this period, temporary bite is formed against the background of the eruption of baby teeth);
- from three to six years (the jaw system is actively developing, preparing for the next stage of eruption);
- from six to twelve years (against the background of mixed bite, the gradual replacement of temporary teeth with permanent ones occurs);
- from twelve to fifteen years (the permanent bite is finally formed).
By the age of about 15, the child's dental arches have fully formed. Normally, the upper and lower rows should be fully closed during chewing. The exception is the first lower incisors (wisdom teeth appear later). A deep bite in a teenager can develop with any disruption in the course of any of the listed stages. It is important for parents to pay attention to the problem in a timely manner, because the child rarely indicates discomfort and makes any complaints about the teeth. It is optimal to visit a pediatric dentist every six months, who will accurately determine pathological changes and will be able to take appropriate measures in a timely manner.
Forms
Dentists have identified two variants of the disorder's manifestation - the dental alveolar and skeletal forms of deep bite. Dental symptoms are the same in both situations. However, with a dental alveolar change, the patient's face looks normal, while with a skeletal form, it has a disproportionate appearance. Deep skeletal bite is less common and requires complex treatment, which should be started in childhood, during the period of active formation of the bone-jaw system. If you do not start treatment procedures in time, then only surgical intervention can help in the future.
Deep bite is divided according to the type of overlap of the frontal row into horizontal and vertical types.
In addition, there are two types of violation: distal and neutral.
A deep distal bite always attracts attention regardless of the patient's age: the chin is reduced and slanted, facial proportions are disturbed. If such a person smiles, the gum surface is noticeably exposed. In turn, a distal bite is divided into two subtypes:
- fan-shaped teeth against the background of narrowing of the lateral row;
- The upper crowns are tilted as much as possible, there is no gap between them.
Another type is a deep neutral bite, which is practically invisible from the outside and does not cause any disturbances in facial proportionality. However, the supramental fold deepens, and when opening the mouth, the lower row overlaps the upper one. Even at a young age, tooth enamel wear is noticeable, and inflammatory processes are often a concern.
Other forms of pathology are of the following types:
- A deep open bite is characterized by the appearance of a gap in the lower-upper direction, which is explained by the non-closure of the lateral and frontal teeth.
- A deep traumatic bite is accompanied by a strong overlap of the crowns, which leads to their cutting edges touching the soft tissues (which, accordingly, are injured).
- Deep incisor bite is the final stage of deep misocclusion, in which complete coronal overlap is observed.
- Deep crossbite is a disordered relationship of the jaws due to the curvature of specific crowns or the entire jaw. There are two types of crossbite:
- deep anterior bite (the upper jaw descends into the lower jaw);
- posterior bite (upper jaw covers the lower jaw).
- A deep prognathic bite involves an abnormal jaw relationship in which the upper jaw protrudes significantly forward in relation to the lower jaw, and there is no contact between the incisors. This defect is classified as a sagittal plane anomaly.
Complications and consequences
The most common negative consequence of a deep bite is a violation of the chewing load, since some teeth experience increased load against the background of inactivity of others. Overloaded teeth are more susceptible to various diseases. Already by about 35 years of age, patients with a deep bite begin to notice a noticeable deterioration in the condition: increased tooth mobility, exposure of roots, abrasion of enamel, bleeding gums are observed. The temporomandibular mechanism also suffers, becoming more vulnerable. Pains in the head, spine (especially in the cervical region) appear, unpleasant sensations arise during eating or sleeping.
With a deep bite, external unaesthetic disorders may also be detected - for example, sunken cheeks, changes in the shape of the lower jaw, early formation of wrinkles. In turn, such changes often become the causes of depression, neurosis, and isolation of patients.
The load on the digestive organs increases, which is associated with insufficient chewing of food. The risk of developing infectious and inflammatory diseases increases (a deep bite sometimes makes it difficult to adequately clean teeth from plaque).
In addition, if the patient has an incorrect bite, the dentist often has difficulty performing treatment and prosthetic procedures.
In general, the most common negative consequences of deep bite can be listed:
- frequent mucosal injuries, chronic stomatitis;
- abnormal chewing, swallowing and breathing functions;
- increased vulnerability and wear of the enamel coating;
- frequent periodontal diseases;
- joint diseases, back and head pain;
- problems with the digestive tract;
- psychological and physical discomfort.
Diagnostics overbite
To diagnose and identify types of deep bite, the dentist determines:
- indicator of the width of the crowns of the lower and upper incisors, their location relative to the axis (correct position, tendency to retrusion or protrusion);
- the degree of expression of the dental upper incisor cusps;
- contact of the front teeth;
- mutual relationship of the canines with the first permanent molars in the sagittal direction (the dental arches are closed in the usual position);
- premature destruction or loss of temporary or permanent lateral teeth;
- mesial inclination, or shift of the row towards a free space as a result of destruction or removal of other teeth;
- the degree of expression of morphofunctional disorders (Siebert-Malygin method) and the complexity of their correction (Malygin-Bely method). [ 7 ]
The appropriate measurements should be taken and calculated:
- mesiodistal index of the crowns of the lower and upper incisors, their total number;
- the degree of compliance of the set of mesiodistal indicators for the crowns of the lower and upper incisors according to the Tonn index (1.35 mm);
- indicator of the depth of overlap of cutters;
- the size of the sagittal space between the central incisors above and below;
- anterior segment length index of the dental arches (Corkhaus method);
- dental arch width indicator (Pont method, Linder and Hart corrections).
The diagnosis is made based on the results of clinical examinations, examination and measurements of the jaws, and metric assessment of photographic facial images from different angles. [ 8 ]
Additionally, teleradiography is performed – X-rays of the skull in different projections. The procedure is performed from a large distance, which allows obtaining a picture close in size to the original object. A special device, orthopantomograph, is used for TRG.
Differential diagnosis
There are several forms of malocclusion in dentistry, and they need to be distinguished. The optimal one is considered to be orthognathic occlusion, when the upper row of teeth slightly overlaps the lower one: this condition is normal and contributes to optimal chewing function.
Other, incorrect types of closures are as follows:
- distal - it is characterized by excessive maxillary development compared to underdevelopment of the lower jaw;
- mesial - characterized by the lower jaw being pushed forward;
- open - observed when the overwhelming majority of teeth in both jaws do not close;
- cross - characterized by underdevelopment of one of the dental rows;
- dystopic - this is a disorder with an incorrect arrangement of teeth, which are not in the right row.
A deep bite is defined as an overbite when the upper row of teeth overlaps the lower row by more than 50% of the height of the teeth. [ 9 ]
Who to contact?
Treatment overbite
Treatment for deep bite is considered more effective if it is started during the periods when temporary teeth are erupting, or the first or second permanent molars, or when temporary incisors are replaced by permanent ones. The doctor sets the following tasks:
- neutralization of the root cause that led to the violation;
- correction of the shape of dental arches and the position of individual teeth;
- stabilization of the mandibular position, normalization of jaw development.
For correction, various methods and techniques are used, taking into account the initial provoking causes and the period of formation of the malocclusion.
If we are talking about temporary deep bite, it is recommended to explain to children the need to chew hard foods (crackers, raw fruits and vegetables) to stimulate adequate jaw development, normal formation of alveolar processes and teeth. If caries is detected affecting temporary molars, they are restored as much as possible. They try to eradicate bad habits, such as biting lips, sucking fingers, etc. This should be done as early as possible, since such habits are not at all harmless for the formation of the bite.
During the period of active bite change – approximately from 5.5 to 9 years – intensive orthodontic correction begins. It is at this time that lateral dental disengagement occurs, which leads to dental alveolar lengthening and contact with the corresponding teeth, so the incisal overlap becomes smaller. If a neutral deep bite is diagnosed, then special removable plates are used for lateral dental disengagement, installed on the upper jaw and having a bite area for the anterior stop, clasps and other fixators. Such a plate is made on a wax base, modeled on the upper jaw and has a thickening in the front, which serves to disengage the lateral teeth a couple of millimeters more than in a physiologically calm state. The plate is fixed with clasps, vestibular arches, or other fixing devices. In order for the lower jaw not to shift forward, left or right, the bite surface must have imprints of the cutting edges of the incisors and tubercles of the canines of the second jaw. In some cases, the plate is equipped with a spring mechanism or a screw-expander.
Sometimes orthodontic aligners are used to correct a deep bite. These transparent caps help correct the disorder unnoticed by others, but they are not always indicated. They can only be used in patients with a simple displacement. Many specialists point out that the effect of treatment with braces and aligners for a deep bite is almost the same. However, wearing aligners is more comfortable - both psychologically for the patient and practically.
Deep bite correction with caps is well tolerated: special pads are made of elastic transparent polymer material, which does not injure soft tissues and is practically not felt in the oral cavity. Caps are able to solve many orthodontic problems at almost any age.
And yet, most often, specialists recommend correcting deep bite with braces, or so-called bracket systems. A special design exerts the necessary pressure, helping to restore the correct position of the dentition. With deep bite, any type of braces can be used - lingual, vestibular, metal, ceramic or ligature-free. The doctor decides which type will be more suitable for a particular person.
Surgical treatment
Often, with a pronounced deep bite, conventional treatment does not bring the desired result. In such cases, doctors advise seeking help from orthodontic surgeons.
Invasive orthognathic surgery includes a number of methods and techniques that make the intervention extremely gentle. All manipulations to correct deep bite and bone defects in an adult patient are performed through the oral cavity, with minimal intensity of the surgeon's movements and with a minimal incision. [ 10 ]
After orthognathic surgery, there are no facial scars, and the result can be observed immediately after the completion of the intervention. The preparation period takes about a month: during this time, the doctor, using special programs, models the necessary manipulations in advance that will be used during surgical treatment. This allows you to minimize the likelihood of risks, as well as shorten the term of the operation. [ 11 ], [ 12 ]
What do patients with deep bite need to know about possible surgical intervention?
- Deep bite correction surgery can be performed from the age of 18, after the completion of the bone growth period.
- The surgical period lasts approximately 1-6 hours, depending on the complexity of the problem.
- The intervention is performed under general anesthesia.
- In the postoperative period, orthodontic therapy will be prescribed with mandatory wearing of braces. The duration of this wearing is determined in a specific order.
After the operation, the patient is given an individual plan for rehabilitation and further orthodontic treatment. [ 13 ]
Exercises
In the case of a simple form of deep bite, the use of various auxiliary means is permitted, which, in particular, include special exercises.
Dentists have developed a set of exercises that are suitable for independent use at home. Exercises should be conducted regularly, since the success of the event depends entirely on this. This set is optimally suitable for children and adolescents, since their jaw-dental system is still in the formation stage. Children are recommended to do exercises under adult supervision.
To correct a deep bite, you need to perform the following manipulations three times a day:
- Open your mouth wide, then gradually close it rhythmically, using short forward movements.
- Touch the roof of your mouth with the tip of your tongue and push your tongue back as far as possible. Keeping your tongue in this position, open and close your mouth.
- Place the elbow of one hand on the table, rest your chin on the palm of the hand. In this position, open and close your mouth (the head should move, but not the lower jaw).
- Repeat the first exercise.
The above exercises are repeated six times one after another. In addition to the exercises, do not forget to load the jaw by regularly chewing hard plant products, which also helps improve the dental row.
This exercise should also be practiced daily. The patient stands up straight, puts his hands behind his back, lifts his chin up. Moves the lower jaw as far away from himself as possible, then returns to the original position. The exercise is repeated three times a day, fifteen times.
Any such activities should be performed with great caution, as excessively intense movements can cause harm and even lead to the need for urgent medical attention.
Myogymnastics for deep bite
In childhood, malocclusion is often associated with abnormal function of the maxillofacial muscles. In order for a child to chew, swallow, breathe and speak normally, the muscles of the mouth and face must be balanced. For example, if a child constantly breathes through the mouth, his mouth is open. This entails excessive tension in the chewing muscles, a change in the width of the jaws and an abnormal formation of the bite. Or, when the swallowing process changes with facial hyperactivity, a gap forms between the front teeth of the child, which entails problems with the quality of speech. Such examples clearly demonstrate the interrelationship of the work of human organs.
In case of deep bite, doctors often prescribe myogymnastics, which is a kind of training of facial muscles. We suggest you consider the main exercises used for such correction.
- The lower jaw is gradually pushed forward until the lower incisors are in front of the upper ones. The position is fixed for ten seconds, after which the initial position is gradually returned.
- They take a wooden stick, stretch a rubber tube over it, and place it between the front teeth. The patient alternately clenches and unclenches his jaws.
To achieve the effect, the exercises are performed twice a day, approximately 12-14 times, daily. However, before starting the gymnastics, you should first consult a dentist.
Prosthetics for deep bite in adults
If the question of dental prosthetics arises, then patients with a deep bite are first sent to an orthodontist to “raise” the height of the bite.
Prosthetics will be performed after orthodontic therapy. In this case, teamwork is used, during which the orthopedic doctor is responsible for the overall treatment concept. He consults with the orthodontist, discussing the desired result. The orthodontist, in turn, analyzes how it can be achieved. Then the orthopedist draws up a scheme of tooth movement and passes it on to the orthodontist.
If the patient already has any orthopedic devices (veneers or crowns) in the oral cavity, then braces can be installed on them. However, after the completion of the orthodontic correction period, such devices are most often replaced due to changes in the bite and shape of the dentition.
After completion of the preliminary treatment, the previously installed temporary crowns are replaced with permanent ones, taking into account the changed bite.
An orthodontic splint – a retainer – is not glued to the orthopedic structure. The exception is veneers: in this situation, the inner side of the tooth is not involved, and the splint will be clearly fixed. Ceramic crowns are a poor basis for gluing a retainer, so in such a case, a retaining cap is used. For a year after the end of treatment, the cap will relieve the load on the front teeth, which stabilizes the therapeutic effect.
Prevention
The formation of an incorrect bite, in particular, a deep bite, starts in early childhood. Therefore, the first rule of prevention should be addressed to parents. And this is especially important if there is a hereditary predisposition to such disorders in the family. Parents should be attentive and contact doctors at the first signs of a problem.
Pregnant women should not only take care of their own health, but also remember that the processes of dental mineralization in the future baby occur at about the 20th week of gestation. Therefore, the second trimester of pregnancy is the period when it is necessary to ensure sufficient calcium and fluoride intake into the body.
From the moment of birth, the baby's nutrition should be extremely balanced and complete. Breastfeeding is, of course, a priority. During the first months after birth, the baby's lower jaw is still in the process of formation, so it is smaller in size than the upper jaw. Breastfeeding causes intensive work of the jaw muscles, which leads to a gradual equalization of the jaw sizes. Artificial feeding does not give the muscles the necessary load, since it is much easier to "get" milk from a nipple.
It is equally important to ensure that the growing baby adheres to nasal breathing and does not have bad habits such as thumb sucking, pacifiers, etc.
And another universal means of preventing the occurrence of deep bite at any age is regular visits to the dentist. The doctor will always pay attention to any violation, monitor the tendency of bite change, recommend the necessary treatment.
Forecast
The duration of the period of correction of deep bite depends on the age at which treatment was started, how severe the disorder was, whether there were other anomalies or dental deformations, whether there were general developmental disorders.
In general, the prognosis is considered favorable, especially if corrective measures were taken at the initial stage of temporary or permanent bite, and during the treatment it was possible to get rid of both morphological and functional disorders. The worst prognosis is expected if deep bite is a genetic feature.
The duration of further use of various retaining (retention) devices after completion of orthodontic therapy depends on the treatment methods used, whether there are any functional disorders that have not been corrected, what positive results have been achieved, and the patient's age. If high-quality dental occlusion has been achieved against the background of adequate functioning, further retention may not be required. If the problem is not completely eliminated, the patient is prescribed appropriate retaining devices, which are selected depending on the most probable expected dental displacement. The duration of use of such devices is individual.
Deep bite and the army
Can a person go to serve in the army if they have a deep bite? Most conscripts think that the quality of the bite does not affect the ability to serve. However, this is not entirely true: some young people are actually refused conscription if the deviation they have is complex and requires medical correction.
So, regardless of the form of malocclusion (deep, distal, etc.), if the indicators deviate greatly from the norm, the conscript may be exempted from military service. For example, this is possible:
- with a deep bite of the second degree and a divergence of 5-10 mm against the background of reduced chewing ability (less than 60%);
- for deep bite of II – III degree, with a divergence of more than 10 mm.
In the latter case, it is especially difficult to go to serve in the army. In most cases, such a conscript is sent for treatment, having previously been granted a deferment from service. Men with a clearly expressed intermaxillary divergence are completely exempt from conscription.
If there are controversial issues with the military commissariat doctors, the fitness category is determined after additional diagnostics. Research is necessary to assess the degree of development of the disorder and the quality of the chewing function. If a pronounced deep bite is confirmed, the conscript is assigned category "B" and given a deferment for treatment and corrective measures.