
All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Cytomegalovirus hepatitis.
Medical expert of the article

Last reviewed: 05.07.2025
Epidemiology
CMV infection is widespread. 70-80% of adults have virus-neutralizing antibodies in their blood. The virus is excreted in urine in 4-5% of pregnant women, in cervical scrapings it is detected in 10% of women, in milk - in 5-15% of nursing mothers. Among newborns who died from various causes, signs of generalized CMV infection are detected in 5-15%. Cytomegalovirus hepatitis accounts for 1% of the etiologic structure of acute icteric hepatitis of viral etiology. However, the prevalence of cytomegalovirus hepatitis as a whole has not been studied to date.
The source of CMV infection is only a person, a sick person or a virus carrier. Transmission occurs by contact, less often - by airborne droplets and enterally. In addition, infection can occur parenterally, including during blood transfusions. This route of transmission is apparently more common than is commonly believed, which is confirmed by the frequent detection of cytomegalovirus in donors (up to 60%). The transplacental route of infection transmission has been reliably proven. Infection of the fetus occurs from the mother - a carrier of the virus. The infection is transmitted directly through the placenta or intrapartum during the passage of the child through the birth canal. Newborns can be infected through their mother's milk.
In cytomegalovirus hepatitis, the predominant routes of infection are apparently parenteral and perinatal, when the cytomegalovirus enters the blood directly, bypassing the patient's lymphoid apparatus.
Causes cytomegalovirus hepatitis
Cytomegalovirus, a member of the Herpesviridae family, was isolated in 1956 by M. Smith. According to modern classification, it is called human herpes virus type 5 (HHV5). Currently, two serotypes of cytomegalovirus are known. Morphologically, it is similar to the herpes simplex virus. The virion contains DNA and has a diameter of 120-140 nm, and is well cultivated in human embryo fibroblast culture. The virus is well preserved at room temperature, is sensitive to ether and disinfectants. It has a weak interferonogenic effect. Cytomegalovirus causes disease exclusively in humans. The fetus and newborns are especially sensitive to the virus.
Pathogens
Pathogenesis
The pathogenesis of cytomegalovirus hepatitis is still unclear. Traditionally, CMV is believed to primarily affect the bile ducts with the development of cholestatic hepatitis. However, a direct cytopathic effect of CMV directly on the liver parenchyma is allowed. Some consider cytomegalovirus to be an undoubted hepatotropic agent. In this case, liver damage can be observed both in congenital and acquired CMV infection.
In the formation of isolated damage to hepatocytes in cytomegalovirus hepatitis, an important role can be played by the direct entry of the pathogen into the blood (parenteral mechanism of infection). In this case, the virus does not enter the lymphatic system, and therefore - into the regional lymph nodes, and even more so does not multiply in them. The pathogen immediately appears in the general bloodstream, from where it enters the liver parenchyma. This phase of the pathogenetic chain can be conventionally called parenchymatous diffusion. In this case, the virus can immediately penetrate into hepatocytes, where it finds conditions for reproduction.
In the pathogenesis of isolated cytomegalovirus hepatitis, the role of different cytomegalovirus genotypes, as well as polymorphism of candidate genes of the major histocompatibility complex (HLA system) on chromosome 6 of a susceptible individual, cannot be excluded.
Pathomorphology
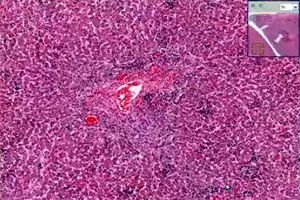
Morphological changes in acute cytomegalovirus hepatitis in healthy adults are characterized by a combination of intralobular granulomas with sinusoidal infiltration by mononuclear cells, as well as periportal inflammation. Hepatocyte necrosis may be mild.
In immunocompromised adults (who have undergone kidney transplantation) with chronic cytomegalovirus hepatitis, periportal and perisinusoidal fibrosis, mixed-cell infiltration, hepatocyte ballooning, and signs of cholestasis are observed. In the earliest stages of the disease, cytomegalovirus antigens in the liver are detected in sinusoidal cells as a result of hematogenous spread of the virus. Necrotic, dystrophic changes in hepatocytes, lymphocytic infiltration, activation of Kupffer cells are noted, while specific cell transformation is rare. Cytomegalovirus hepatitis in these patients is accompanied by cholestatic syndrome and bile duct disappearance syndrome. In this case, pp65 antigenemia and CMV DNA are detected in hepatocytes, and signs of liver cirrhosis may be observed.
In addition to the classic changes characteristic of viral hepatitis, patients with cytomegalovirus liver damage may have small aggregates of neutrophilic polymorphonuclear leukocytes, often located around the infected hepatocyte with intranuclear CMV inclusions. Immunohistochemistry methods have revealed that basophilic granularity of the cytoplasm in cells without classic intranuclear CMV inclusions is caused by the presence of cytomegalovirus material. Thus, not only intranuclear inclusions of the virus, but also basophilic granularity of the cytoplasm are a characteristic sign of CMV hepatitis.
In general, in immunocompromised patients, CMV infection has a more pronounced cytopathogenic effect and causes more extensive lysis of hepatocytes than in immunocompetent patients with CMV hepatitis.
Morphological changes in liver tissue in children with congenital CMV hepatitis are characterized by giant cell transformation of hepatocytes, cholestasis, portal fibrosis, proliferation of the bile duct epithelium, and in cases of fulminant forms, massive liver necrosis.
Symptoms cytomegalovirus hepatitis
Cytomegalovirus hepatitis can have both acute and chronic course.
 [ 23 ]
[ 23 ]
Acute acquired cytomegalovirus hepatitis
Acquired acute CMV hepatitis in children, adolescents and young adults can be diagnosed within the symptom complex of infectious mononucleosis. However, in some cases, isolated liver damage is observed. In this case, the disease occurs in anicteric, mild, moderate or severe form. In isolated cases, fulminant hepatitis can develop.
The incubation period for CMV hepatitis has not been precisely established. It is presumably 2-3 months.
Preicteric period. Clinical manifestations and laboratory parameters in acute CMV hepatitis are not fundamentally different from those in viral hepatitis of other etiologies. The disease begins gradually. Patients experience decreased appetite, weakness, headache, abdominal pain. In some cases, body temperature rises to 38 °C,
The duration of the pre-icteric period of acute CMV hepatitis A usually ranges from 3 to 7 days.
Clinical manifestations of the pre-icteric period may be absent. In such cases, the manifest initial form of cytomegalovirus hepatitis debuts with the appearance of jaundice.
Jaundice period. In patients after the onset of jaundice, the symptoms of intoxication observed in the pre-jaundice period persist or even increase.
Clinical and laboratory manifestations of acute cytomegalovirus hepatitis are not fundamentally different from those of viral hepatitis of other etiologies.
The duration of the icteric period in acute cytomegalovirus hepatitis ranges from 13 to 28 days.
The post-icteric period of the disease is characterized by normalization of the patient's well-being, a decrease in the size of the liver and spleen, and a significant decrease in enzyme activity.
Chronic cytomegalovirus hepatitis
Chronic cytomegalovirus hepatitis most often develops in immunocompromised patients (infected with HIV, receiving immunosuppressive therapy, having undergone liver transplantation, etc.). Thus, cytomegalovirus graft damage is observed in 11-28.5% of patients who have undergone liver transplantation for various reasons (autoimmune liver diseases, viral hepatitis, etc.). CMV DNA is detected in the hepatocytes of 20% of liver transplant recipients with a clinical, biochemical and histological picture of hepatitis.
However, the development of chronic cytomegalovirus hepatitis is also possible in immunocompetent children and adults. In this case, chronic hepatitis can develop as a primary chronic process or as a result of initial manifest cytomegalovirus hepatitis.
Clinical and laboratory parameters in patients with acquired chronic CMV hepatitis do not differ fundamentally from those observed in chronic viral hepatitis of other etiologies.
In patients with acquired chronic CMV hepatitis, low and moderate activity of the process predominates. In almost 3/4 of cases, moderate and severe liver fibrosis is diagnosed.
During the remission period, intoxication symptoms in patients with acquired chronic CMV hepatitis are practically absent. Extrahepatic manifestations disappear in most patients. The liver and spleen shrink in size, but their full normalization is not observed. Usually, the edge of the liver protrudes from under the costal arch by no more than 1-2 cm. The spleen is palpated less than 1 cm below the edge of the costal arch. Enzyme activity in the blood serum does not exceed normal values.
Clinical manifestations of acquired cytomegalovirus hepatitis correspond to those of acute and chronic viral hepatitis of varying severity. In 3/4 cases of acquired chronic cytomegalovirus hepatitis, moderate and severe liver fibrosis is diagnosed.
[ 26 ], [ 27 ], [ 28 ], [ 29 ], [ 30 ]
Congenital cytomegalovirus hepatitis
Congenital CMV infection can occur both in a generalized form with damage to many organs and systems, and in localized forms, including the liver. Liver damage is typical for congenital CMV infection and occurs in 40-63.3% of patients. Changes in the liver include chronic hepatitis, cirrhosis, cholangitis, intralobular cholestasis. Damage to the extrahepatic biliary tract, from inflammation to atresia, is recorded. To date, the role of cytomegalovirus in the genesis of damage to the extrahepatic biliary tract (atresia, cysts) remains unclear.
Congenital cytomegalovirus hepatitis is registered mainly in children of the first months of life, proceeds either in anicteric form with hepato-splenomegaly and biochemical activity, or in an icteric form with icterus, dark urine, hepatosplenomegaly, hypertransaminasemia, increased levels of alkaline phosphatase and GGT, the formation of liver cirrhosis in half of the patients. At the same time, congenital cytomegalovirus hepatitis can proceed in the form of acute and protracted forms with one- or two-wave jaundice, mild manifestations of intoxication, activity of hepatocellular enzymes increased by 2-3 times, cholestatic syndrome (in 1/3 of patients), rarely taking a chronic course, which in these cases develops as a primary chronic process occurring without jaundice and with moderate or high pathological activity.
[ 31 ], [ 32 ], [ 33 ], [ 34 ], [ 35 ], [ 36 ], [ 37 ]
Congenital primary chronic cytomegalovirus hepatitis
Among children with congenital chronic CMV hepatitis, minimal activity of the pathological process in the liver is diagnosed in 1/4 of cases, low activity in 1/3 of cases, and moderate activity in 1/3 of patients.
The process has a pronounced fibrosis-generating direction. In 1/3 of patients, pronounced fibrosis is diagnosed, in 1/3 - signs of liver cirrhosis.
Clinical manifestations and laboratory parameters in congenital chronic CMV hepatitis do not have fundamental differences from viral hepatitis of other etiologies.
During the remission period, intoxication symptoms in patients with congenital chronic CMV hepatitis are practically absent. Extrahepatic manifestations disappear in most children. The liver and spleen shrink in size, but their full normalization is not observed. Usually, the edge of the liver protrudes from under the costal arch by no more than 1-2 cm. The spleen is palpated less than 1 cm below the edge of the costal arch in most patients with splenomegaly. Enzyme activity in the blood serum does not exceed normal values.
Cytomegalovirus hepatitis in liver transplant patients
Cytomegalovirus hepatitis is the most common manifestation of CMV infection against the background of immunosuppressive therapy. In such cases, the diagnosis of cytomegalovirus hepatitis is established based on the results of liver biopsy and confirmed by the method of viral culture, ppb5 antigen, PCR, and immunohistochemistry. Most patients with CMV hepatitis develop isolated liver damage, and only a few patients develop generalized CMV infection. Patients are prescribed intravenous ganciclovir. In AIDS, cytomegalovirus hepatitis is observed in 3-5% of patients.
In patients who have undergone orthotopic liver transplantation and in AIDS, it is possible to develop strictures of the extrahepatic bile ducts of cytomegalovirus etiology, which is confirmed by the detection of the virus B in the epithelium of the bile ducts. Infection of the donor and recipient of the liver with cytomegalovirus before transplantation is considered a factor contributing to transplant rejection.
[ 41 ], [ 42 ], [ 43 ], [ 44 ], [ 45 ], [ 46 ]
The course of cytomegalovirus hepatitis
The course of the disease can be acute (35%) and end in recovery with complete restoration of the functional state of the liver within 1 to 3 months. In 65% of patients, as a result of manifest cytomegalovirus hepatitis, the disease becomes chronic.
Where does it hurt?
Diagnostics cytomegalovirus hepatitis
Cytomegalovirus hepatitis is diagnosed based on a combination of clinical, biochemical and serological data. The disease usually begins with astheno-dyspeptic manifestations: malaise, weakness, loss of appetite, accompanied by an increase in the size of the liver and hyperfermentemia. The patient's history may indicate parenteral manipulations 2-3 months before the current disease, there are no markers of hepatitis viruses A, B, C, U, G, etc. in the blood serum.
It is important to consider that cytomegalovirus hepatitis is characterized by a pronounced cytolysis syndrome. For its indication, determination of aminotransferase activity (ALT, AST) and LDH fractions (LDH-4, LDH-5) is widely used. Increased activity of liver cell enzymes is characteristic of acute hepatitis and the exacerbation stage of chronic cytomegalovirus hepatitis. The degree of increase in the activity of liver cell enzymes in various forms of cytomegalovirus hepatitis corresponds to that in viral hepatitis of other etiologies.
In the presence of jaundice, it is important to determine the level of total bilirubin and the ratio of conjugated and unconjugated fractions.
The activity of the inflammatory process in the liver is reflected to a certain extent by the protein spectrum of the blood serum. In most cases, patients with chronic CMV hepatitis maintain a normal level of total protein in the blood serum - 65-80 g / l. In patients with chronic CMV hepatitis of high activity, dysproteinemia is formed due to a decrease in the level of albumins and an increase in the fraction of y-globules and novae. The nature of dysproteinemia is moderate and reaches significant expression only in some patients, when the albumin level falls below 45%, and the level of y-globulin exceeds 25%.
During exacerbation of chronic cytomegalovirus hepatitis, the decrease in protein-synthetic function is more significant, the more severe the inflammatory process in the liver. Disorders in the blood coagulation system (hypocoagulation) of varying degrees develop in patients with chronic hepatitis mainly due to a decrease in the synthetic function of the liver.
The ultrasound picture in the liver in acute and chronic CMV hepatitis is no different from that in viral hepatitis of other etiologies.
The Doppler ultrasound method is used to determine blood flow in the portal vein system and the presence of portocaval anastomoses, which allows for the diagnosis of portal hypertension, including in patients with liver cirrhosis of cytomegalovirus etiology.
Morphological studies allow an objective assessment of the nature of the pathological process in the liver, its direction, and also serve as one of the mandatory criteria for the effectiveness of the therapy.
The results of a puncture biopsy can have a decisive differential diagnostic value. With a sufficient size of the liver puncture, the obtained morphological information is of decisive importance in assessing the activity, degree of fibrosis of chronic hepatitis and in choosing therapeutic tactics.
What do need to examine?
Who to contact?
Treatment cytomegalovirus hepatitis
Ganciclovir and recombinant interferon A preparations are used to treat cytomegalovirus hepatitis.
Below are the results of one clinical study, which treated 85 children who received Viferon therapy for chronic cytomegalovirus hepatitis. Among them, 31 children had acquired and 54 had congenital CMV hepatitis. In 49 children, congenital cytomegalovirus hepatitis was combined with damage to the biliary system (in 44 - atresia and in 5 - cysts of the bile ducts), and in five - with damage to the central nervous system.
Among the observed patients there were 47 boys and 38 girls. 55 children were under 1 year of age, 23 were 1 to 3 years old, and 7 were over 3 years old.
For the course of chronic viral hepatitis, 45 children received monotherapy with Viferon in rectal suppositories, 31 - Viferon in combination with intravenous immunoglobulins, 9 children - combination therapy consisting of Viferon and ganciclovir. The dose of interferon is 5 million/m2 , 3 times a week.
The duration of the treatment course was 6 months in 67 patients, 9 months in 11 and 12 months in 7 children. The criteria for the effectiveness of interferon therapy were determined in accordance with the EUROHEP consensus.
The control group consisted of 43 children. It included 29 patients with congenital and 14 with chronic hepatitis of cytomegalovirus etiology. These children received basic therapy, including only choleretic, vitamin preparations and hepatoprotectors.
In addition to clinical and biochemical monitoring, the replicative activity of cytomegalovirus was verified during the course of the disease.
The proportion of children with chronic CMV hepatitis who achieved complete remission against the background of viferon therapy was low and did not reach 20%. However, the combined group of children who had some remission constituted 78.8% of the total number of treated children. At the same time, remission was absent in almost 1/4 of the patients. It should also be noted that spontaneous remission did not develop in any child from the control group within the same time frame.
A comparative analysis of the effectiveness of viferon therapy in children with congenital and acquired CMV hepatitis showed that no reliable differences in the percentage of remission formation were found against the background of viferon therapy. The p values ranged from p>0.05 to p>0.2.
In order to answer the question about the dependence of the frequency of achieving remission in cytomegalovirus hepatitis during therapy on the treatment regimen, 3 groups were identified. The first included patients who received monotherapy with Viferon, the second - children who received Viferon in combination with intravenous immunoglobulins, and the third - those who received combined therapy with Viferon and ganciclovir.
No significant differences in treatment results were found in patients from different groups. Only a tendency toward lower cytolysis severity was noted in children with combined treatment with Viferon and intravenous immunoglobulins. The p values ranged from p>0.05 to p>0.1.
A similar pattern is also observed when assessing the replicative activity of CMV in chronic cytomegalovirus hepatitis in children who received various treatment regimens. The frequency of CMV DNA detection during dynamic observation was virtually identical in children from all three groups. Only slightly lower replicative activity of CMV was observed in patients treated with Viferon in combination with intravenous immunoglobulins. The p values ranged from p>0.05 to p>0.2.
More information of the treatment
Prevention
Specific prevention of CMV infection has not been developed. Experimental work is underway to create a vaccine.
Anti-epidemic measures are not carried out in foci of infection. Given the potential role of the parenteral mechanism of infection in the formation of cytomegalovirus hepatitis, measures to suppress all possibilities of parenteral, including transfusion, infection seem especially important. The use of disposable needles, compliance with the rules for sterilization of surgical instruments can completely prevent infection during parenteral manipulations.
To prevent infection with cytomegalovirus during transfusions of blood and its components, it is necessary to decide on testing donor blood for CMV DNA.