
All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Pierre Robin syndrome
Medical expert of the article

Last reviewed: 04.07.2025

Pierre Robin syndrome, also known in medicine as Robin anomaly, is a congenital pathology of the development of the jaw part of the face. The disease received its name in honor of the French dentist P. Robin, who first described all its signs. Lannelongue and Menard first described Pierre Robin syndrome in 1891 in their report on two patients with micrognathia, cleft palate and retroglossoptosis. In 1926, Pierre-Robin published a case of the disease in an infant with signs of the classic syndrome. Until 1974, the triad of signs was known as Robin-Pierre syndrome. However, this syndrome is now used to describe malformations with the simultaneous presence of multiple anomalies.
Epidemiology
It is a heterogeneous congenital defect that has a prevalence of 1 in 8,500 live births. The male to female ratio is 1:1, except for the X-linked form.
Among these patients, 50% of infants have an incomplete cleft soft palate, the rest are born with an arched and unusually high palate, but without a cleft.
Causes Pierre Robin syndrome
The possibility of autosomal recessive inheritance of the disease is considered. There are two types of syndrome depending on the etiology: isolated and genetically determined. The isolated type develops due to compression of the lower part of the jaw during embryonic development. Compression can develop due to:
- The presence of localized seals in the uterus (cysts, scars, tumors).
- Multiple pregnancy.
Also, the development of the jaw in the fetus can be disrupted by:
- Viral infections that the expectant mother suffered during pregnancy.
- Neurotrophic disorders.
- Insufficient amount of folic acid in the body of a pregnant woman.
Pathogenesis
Pierre Robin syndrome is caused by embryonic disorders that are caused by a wide variety of pathologies in the prenatal period.
There are three pathophysiological theories that may explain the occurrence of Pierre Robin syndrome.
Mechanical Theory: This theory is the most likely. Underdevelopment of the mandibular apparatus occurs between the 7th and 11th weeks of pregnancy. The high position of the tongue in the oral cavity leads to the formation of clefts in the palate, due to which the vena cava does not close. This theory explains the classic inverted U-shaped cleft and the absence of the associated cleft lip. Oligohydramnios may play a role in the etiology, since the absence of amniotic fluid can lead to deformation of the chin and subsequent compression of the tongue between the vena cava.
Neurological theory: Delay in neurological development has been noted with electromyography of the muscles of the uvula and pharyngeal columns, and taste due to conduction delay in the hypoglossal nerve.
Theory of dysneuroregulation of the rhombencephalon: This theory is based on the disruption of the development of the rhombencephalon during ontogenesis.
Insufficient development of the lower part of the child's jaw leads to the oral cavity being significantly reduced. This, in turn, causes the so-called pseudomacroglossia, i.e. the tongue is displaced to the back of the pharyngeal wall. This pathology leads to the development of airway obstruction.
As long as the baby cries or moves, the airway remains clear, but as soon as the baby falls asleep, obstruction occurs again.
Due to respiratory disorders, the process of feeding the baby is very difficult. At this time, airway obstruction almost always occurs. If no medical correction is applied, such a pathology can lead to severe exhaustion of the entire body and even death.
Symptoms Pierre Robin syndrome
The disease is characterized by three main symptoms:
- Lower micrognathia (underdevelopment of the lower jaw, occurs in 91.7% of cases of the disease). It is characterized by the retraction of the lower dental arch by 10-12 mm behind the upper arch. The lower jaw has a small body, an obtuse angle. The child achieves normal development at approximately 5-6 years of age.
- Glossoptosis (retraction of the tongue due to its insufficient development, observed in 70-85% of cases).
- Macroglossia and ankyloglossia are relatively rare symptoms, observed in 10-15% of cases.
- A crack appears in the sky.
- Bradypnea and dyspnea.
- Mild cyanosis.
- Asphyxia, which most often occurs during attempts to feed the baby.
- Swallowing is impossible or very difficult.
- Feeling like vomiting.
- Auricular anomalies in 75% of cases.
- Conductive hearing loss occurs in 60% of patients, while atresia of the external auditory canal occurs in only 5% of patients, insufficient pneumatization of the mastoid cavity of the temporal bone.
- Inner ear anomalies (aplasia of the lateral semicircular canals, great vestibular aqueduct, loss of cochlear hair cells).
- Nasal malformations are uncommon and consist mainly of anomalies of the nasal root.
- Dental malformations occur in 30% of cases. Laryngomalacia and velopharyngeal insufficiency occur in approximately 10-15% of patients with Pierre Robin syndrome.

Systemic features of Pierre Robin syndrome
Systemic developmental anomalies are described in 10-85% of registered cases.
Eye abnormalities occur in 10-30% of patients. They may include: hyperopia, myopia, astigmatism, corneal sclerosis and stenosis of the nasolacrimal duct.
Cardiovascular pathologies: benign heart murmurs, pulmonary artery stenosis, patent ductus arteriosus, oval window, atrial septal defect and pulmonary hypertension. Their prevalence varies from 5-58%.
Anomalies related to the musculoskeletal system (70-80% of cases): syndactyly, dysplastic phalanges, polydactyly, clinodactyly, hypermobility of joints and oligodactyly of the upper limbs. Anomalies of the lower limbs: foot anomalies (clubfoot, metatarsal adduction), femoral malformations (valgus or varus pelvis, short femurs), hip anomalies (congenital dislocation, contractures), knee joint anomalies (GENU VALGUS, synchondrosis). Malformations of the spinal column: scoliosis, kyphosis, lordosis, vertebral dysplasia, agenesis of the sacrum and coccygeal sinus.
Central nervous system pathology: epilepsy, delays in the development of the nervous system, hydrocephalus. The frequency of CNS defects is about 50%.
Genitourinary anomalies: undescended testicles (25%), hydronephrosis (15%), and hydrocele (10%).
Associated syndromes and conditions: Stickler syndrome, trisomy 11q syndrome, trisomy 18, 4q deletion syndrome, rheumatoid arthropathy, hypochondroplasia, Moebius syndrome.
Stages
There are three stages of disease severity, which depend on the condition of the child's respiratory tract:
- Mild - there are minor problems with feeding, but breathing is almost not difficult. Treatment is carried out on an outpatient basis.
- Moderate – breathing is moderately difficult, feeding the child is moderately difficult. Treatment is carried out in a hospital.
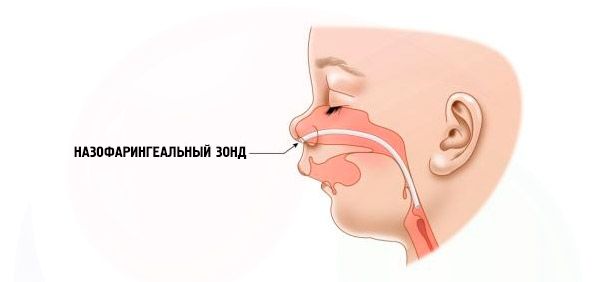
- Severe – breathing is very difficult, the child cannot be fed normally. It is necessary to use special devices (intranasal probe).
Complications and consequences
The combination of micrognathia and glossoptosis can lead to severe respiratory complications and problems during feeding the child.
Pierre Robin syndrome causes the following complications:
- Stridose breathing due to airway obstruction. Laryngomalacia or even sleep asphyxia.
- The child's psychomotor development lags far behind his peers.
- Physical development also lags behind.
- The patients' speech is impaired.
- Frequent ear infections that become chronic and lead to hearing impairment.
- Obstructive sleep apnea syndrome, the occurrence of death in sleep varies in 14-91% of cases.
- Problems with teeth.
Diagnostics Pierre Robin syndrome
Diagnosis of Pierre Robin syndrome is not difficult. It is based on clinical manifestations. To exclude other pathologies, it is very important to consult a geneticist.
Children with Robin's congenital anomaly have breathing problems from birth due to the tongue constantly sinking back. The baby is restless, his skin is bluish, wheezing comes out of the chest when inhaling. Choking may occur during feeding. The diagnosis can also be made by the unusual appearance of the child - "bird face". Often, patients develop other defects: myopia, cataracts, pathology of the genitourinary system, heart pathology, anomalies in the development of the spine.
Based on these clinical manifestations, it will not be difficult for a specialist to make a correct diagnosis.
Who to contact?
Treatment Pierre Robin syndrome
Treatment is carried out immediately after the birth of a child with Pierre Robin syndrome. If the disease is mild, then to improve the patient's condition it is necessary to constantly hold the child vertically or lying on the tummy. The baby's head should be tilted to the chest. During feeding, it is not recommended to hold the child in a horizontal position so that food does not get into the respiratory tract.
If the underdevelopment of the lower jaw is quite pronounced, surgical intervention is used to bring the retracted tongue into a normal physiological position. In severe cases, the tongue is pulled up and fixed on the lower lip. In very severe cases, tracheostomy, glossopexy, and distraction osteogenesis of the lower jaw must be performed.
Conservative treatment is also used.
Medicines
Phenobarbital. A sleeping pill and sedative drug, has an anticonvulsant effect. Each tablet contains 100 ml of phenobarbital. The dosage is individual, as it depends on the severity of the disease and the child's condition. The drug is prohibited for patients with liver failure, hyperkinesis, anemia, myasthenia, porphyria, diabetes mellitus, depression, and intolerance to the components. The following symptoms are possible when taking it: dizziness, asthenia, hallucinations, agranulocytosis, nausea, low blood pressure, and allergies.
Clonazepam. A drug prescribed for the treatment of epilepsy. The drug contains the active substance clonazepam, which is a benzodiazepine derivative. It has anticonvulsant, anxiolytic and muscle relaxant effects. The dose is determined by the attending physician, but should not exceed the maximum - 250 mcg per day. Do not take in case of insomnia, muscle hypertonia, psychomotor agitation, panic disorders. The following symptoms are possible when taking: lethargy, nausea, dysmenorrhea, headache, leukopenia, urinary retention or incontinence, alopecia, allergy.
Sibazon. Available in the form of a solution and rectal tablets. The active substance is a benzodiazepine derivative (sibazon). It has a sedative, anxiolytic, anticonvulsant effect. The dosage is individual. Patients with chronic hypercapnia, myasthenia, benzodiazepine intolerance are prohibited from taking the drug. When using the drug, the following symptoms may develop: nausea, constipation, headache, dizziness, hiccups, urinary incontinence, allergies.
Cortexin lyophilisate. A drug with a nootropic effect. The drug contains a complex of water-soluble polypeptide fractions and glycine. The dosage is individual and is prescribed by the attending physician in accordance with the patient's condition. Patients with intolerance to cortexin are prohibited from taking the drug. The drug may cause allergic reactions.
Physiotherapy treatment
Typically, in mild stages of the syndrome, positional therapy is used, where the child is placed on his stomach in an upright position until gravity forces the lower jaw to grow correctly.
Surgical treatment
Surgical treatment is used primarily to correct glossoptosis. There are several methods:
- Support of the tongue with a silver thread. The thread is passed through the lower part of the gum and the lower lip. The method is called Douglas.
- Duhamel's method - a thick silver thread is passed through the base of the patient's tongue and both cheeks. Use for no longer than thirty days.
- Orthopedic devices for tongue extension and fixation.
- At one year of age, surgery to correct a cleft palate can be performed.
Forecast
The prognosis and course of the disease are severe. Most often, death occurs in the first days of life at the moderate and severe stage of the disease (the cause is asphyxia). Also, the risk of death in the first year is quite high due to numerous infections.
For patients over two years of age, the prognosis is favorable.
 [ 36 ]
[ 36 ]