
All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
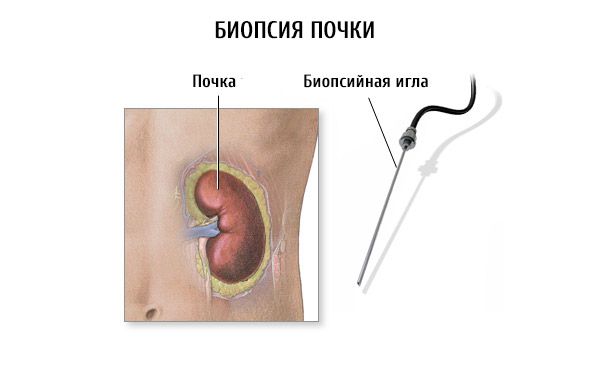
Kidney biopsy
Medical expert of the article

Last reviewed: 04.07.2025

Biopsy is a lifetime morphological study of tissue.
Kidney biopsy is used to diagnose kidney disease and determine treatment tactics. Diagnostic kidney biopsy is used after the possibilities of other, less invasive instrumental methods have been exhausted, including biopsy of the rectal mucosa, nasopharynx, skin, and lymph node.
 [
[ Indications for kidney biopsy
It is necessary to clarify the causes of massive organic proteinuria, primarily nephrotic syndrome, renal hematuria, hypertension, tubulopathy. Biopsy allows to differentiate between primary (Bright) nephritis and nephropathy within the framework of systemic and metabolic diseases, vasculitis, amyloidosis, to establish the type of amyloid, which is important in connection with differentiated therapy of primary and secondary amyloidosis. In case of kidney damage (microhematuria, nephrotic, acute nephritic syndrome ), which joined in the first years of the disease non-insulin-dependent diabetes mellitus, as a rule, it is necessary to perform a kidney biopsy. The prognosis of hypertension, persisting after severe nephropathy of pregnancy, largely depends on the morphological variant of nephropathy: endotheliosis, focal segmental glomerulosclerosis, sclerosis of the interlobular arteries.
Renal biopsy is indicated in renal acute renal failure of unclear etiology. At the same time, it radically changes the diagnosis and therapeutic tactics in more than half of patients with renal acute renal failure, revealing rapidly progressive glomerulonephritis (14%) requiring immunosuppressive therapy, allergic acute tubulointerstitial nephritis (11%), necrotizing vasculitis (20%). Of great practical importance is the distinction between drug-induced acute tubulointerstitial nephritis requiring glucocorticoid therapy and drug-induced prerenal acute renal failure, drug-induced acute tubular and cortical necrosis, intratubular block.
Kidney biopsy largely determines the overall strategy of renal therapy. In ischemic kidney disease and other renovascular hypertension, the results of kidney biopsy allow choosing the tactics of surgical treatment - renal artery angioplasty or nephrectomy. Nephrobiopsy allows detecting relative contraindications to kidney transplantation, it is carried out in patients with chronic renal failure on HD in preparation for kidney transplantation. Often recur and damage the transplant early antibody-based chronic glomerulonephritis, hemolytic uremic syndrome, focal segmental glomerulosclerosis, mesangiocapillary glomerulonephritis. In hepatorenal failure, liver transplantation is effective when kidney biopsy confirms the diagnosis of hepatorenal syndrome or acute tubular necrosis (ATN). In cases where signs of diffuse fibroplastic nephritis are detected against the background of active chronic hepatitis with HBV (HCV) replication, a liver and kidney transplant is necessary.
Diagnostic indications for kidney biopsy
Disease |
Indications for kidney biopsy |
Nephropathy Renal acute renal failure Renal transplant diseases |
Organic proteinuria, nephrotic syndrome, glomerular hematuria, renal hypertension of unknown origin, tubulopathy of unknown origin Unclear etiology, with systemic manifestation, symptoms of glomerulonephritis and vasculitis, anuria for more than 3 weeks Acute cessation and rapid decline in function, increasing proteinuria and hypertension |
Diagnostic biopsy of the kidney transplant is widespread, the causes of its dysfunction are diverse. Acute renal rejection crisis is differentiated from acute drug-induced nephrotoxicity caused by calcineurin inhibitors, antibiotics, NSAIDs, post-transplant lymphoproliferative syndrome, viral acute tubulointerstitial nephritis ( cytomegalovirus ), relapse of glomerulonephritis in the transplant. In 30% of cases, a subclinical variant of acute rejection crisis develops, diagnosed mainly by kidney biopsy, while the morphological variant of the crisis (interstitial, vascular) largely determines the prognosis and treatment tactics.
A kidney biopsy for the purpose of choosing a therapy and monitoring the effectiveness of treatment should be performed in the first 2 years of chronic glomerulonephritis with the obligatory use of immunoluminescent and electron microscopic methods of analysis. Establishing the morphological variant of chronic glomerulonephritis with an assessment of the activity of the renal process and the severity of fibroplastic transformation allows choosing the optimal method of immunosuppressive therapy and predicting its effectiveness ("Glomerulonephritis"). Repeated biopsies monitoring the effectiveness of therapy are performed in patients with active chronic glomerulonephritis (rapidly progressing glomerulonephritis) and in kidney transplant recipients; they are performed from one to 4-6 times a year depending on the severity of the renal process and the characteristics of the therapy. With effective treatment of the rejection crisis, positive morphological changes in the biopsy are several days ahead of the development of biochemical dynamics.
Preparing for a kidney biopsy
Before performing a biopsy, it is necessary:
- assess the state of the blood coagulation system (bleeding time, blood platelet count, coagulogram );
- determine blood type and Rh factor;
- determine the total and individual functional capacity of the kidneys, their location, mobility (intravenous urography).
Intravenous urophagia is performed with the patient lying down and standing.
If there are contraindications to intravenous urography, dynamic renoscintigraphy and echography are used. Ultrasound allows to determine the depth of the kidneys and diagnoses such contraindications to nephrobiopsy as polycystic disease, nephrocalcinosis, radiolucent renal stones.
Before the biopsy, anemia (Ht over 35%) and arterial pressure should be corrected. In case of severe arterial hypertension at the time of biopsy and for 2-3 days after it, controlled hypotension is used by intravenous drip administration of diazoxide, sodium nitroprusside or trimethophan camsylate. In a dialysis patient, a kidney biopsy should be performed no less than 6 hours after the next HD; the next HD session is allowed to be performed no earlier than 24 hours after the biopsy.
Kidney biopsy technique
Kidney biopsy is performed using a closed (percutaneous puncture) or surgical (open, semi-open biopsy) method.
Since the early 80s, a closed kidney biopsy technique has been used under the control of sectoral ultrasound scanning in real time. In kidney biopsy in patients with excess body weight, computed tomography is more effective than ultrasound control.
If complete correction of hypertension, hemorrhagic syndrome and hypocoagulation cannot be achieved, transjugular endoscopic kidney biopsy or open kidney biopsy is used. The method of obtaining a biopsy depends on the structure of the puncture needle. Along with the traditional manual method, automatic biopsy needles are increasingly used.
Ultrasound monitoring of the punctured kidney is performed immediately after the biopsy. To prevent complications, the patient lies on an ice pack for 3 hours after the puncture, and is on strict bed rest for the next 2 days. Hemostatic drugs (menadione sodium bisulfite, calcium chloride) and antibiotics (macrolides or semisynthetic penicillins) are prescribed.
Contraindications to kidney biopsy
Absolute contraindications to kidney biopsy and methods of their diagnosis are reflected in the table.
Relative contraindications:
- uncontrolled hypertension;
- severe renal failure (blood creatinine more than 0.44 mmol/l);
- hypocoagulation;
- thrombocytopenia;
- widespread atherosclerosis;
- severe nephrocalcinosis;
- periarteritis nodosa;
- myeloma nephropathy;
- pathological mobility of the kidney;
- the days preceding menstruation in women.
Absolute contraindications to kidney biopsy and methods of their diagnosis
Contraindications |
Diagnostic methods |
The only functioning kidney Hydronephrosis, polycystic disease Kidney tumor, renal pelvis tumor Renal artery aneurysm Renal vein thrombosis Chronic heart failure Novocaine intolerance Mental inadequacy |
Chromocystoscopy, dynamic scintigraphy, intravenous urography Ultrasound, intravenous urography, computed tomography Ultrasound, intravenous urography, computed tomography Ultrasound Dopplerography, renal angiography Ultrasound Dopplerography, renal venography Echocardiography (EchoCG), measurement of central venous pressure, blood flow velocity Allergic history Consultation with a neuropsychiatrist |
Complications of kidney biopsy
The incidence of serious complications after kidney biopsy is 3.6%, the incidence of nephrectomies is 0.06%, and the mortality rate reaches 0.1%.
- In 20-30% of cases, microhematuria is observed, which persists for the first 2 days after the biopsy.
- Macrohematuria is observed in 5-7% of cases. It is usually short-term and asymptomatic. Long-term macrohematuria, usually caused by renal infarction, is often accompanied by renal colic, tamponade of the bladder with blood clots, which requires urological care.
- Massive bleeding under the renal capsule or into the paranephric tissue with the formation of a perirenal hematoma is characterized by intense constant pain in the lower back, decreased blood pressure and blood hemoglobin levels. Transient cessation of kidney function, compressed by the hematoma, is possible. Hematoma is diagnosed by ultrasound and CT. The choice of treatment for perirenal hematoma (surgical or conservative hemostatic therapy) is carried out together with a urologist.
- Rare, extremely serious complications of kidney biopsy include:
- infection of the hematoma with the development of purulent post-biopsy paranephritis;
- kidney rupture;
- injuries to other organs (liver, spleen, pancreas);
- damage to large vessels (aorta, inferior vena cava).